Вам также может понравиться
- 2 02-Electrocardiography PDFДокумент17 страниц2 02-Electrocardiography PDFMiguel DomingoОценок пока нет
- AntibioticsДокумент9 страницAntibioticsprince1500100% (1)
- Abx FinalДокумент3 страницыAbx Finalyanks1120Оценок пока нет
- Inhibitor of Cell Wall Synthesis (ICWS) : Proteus ComboДокумент12 страницInhibitor of Cell Wall Synthesis (ICWS) : Proteus Comboflomax23100% (1)
- Drug ChartДокумент8 страницDrug Chartstudentalwaysstudy100% (1)
- Adult Infectious Disease Bulletpoints HandbookОт EverandAdult Infectious Disease Bulletpoints HandbookРейтинг: 4.5 из 5 звезд4.5/5 (9)
- Antibacterials CMДокумент72 страницыAntibacterials CMMike AnnisОценок пока нет
- Anti Infective AgentsДокумент42 страницыAnti Infective AgentsDthird Mendoza ClaudioОценок пока нет
- Antibiotics Made EasyДокумент116 страницAntibiotics Made EasyShalini Soorya100% (3)
- Chemotherapy AntibioticsДокумент23 страницыChemotherapy AntibioticsMubarak Abubakar yaroОценок пока нет
- Physiotherapy Scoliosis-Specific Exercises - A Comprehensive Review of Seven Major SchoolsДокумент52 страницыPhysiotherapy Scoliosis-Specific Exercises - A Comprehensive Review of Seven Major SchoolsAmi ZofotaОценок пока нет
- Generic Name Brand Names Common Uses Possible Side Effects Mechanism of ActionДокумент13 страницGeneric Name Brand Names Common Uses Possible Side Effects Mechanism of Actionangel3424Оценок пока нет
- Chemotherapeutic DrugsДокумент122 страницыChemotherapeutic Drugsdex7reme100% (1)
- DYSPHAGIAДокумент47 страницDYSPHAGIANur Khairah AmalinaОценок пока нет
- Antimicrobial AgentsДокумент3 страницыAntimicrobial AgentsErnie G. Bautista II, RN, MD100% (2)
- Case 2 - Acute Back PainДокумент4 страницыCase 2 - Acute Back PainJohn Fightakis100% (1)
- Post-Mortem ExaminationДокумент7 страницPost-Mortem ExaminationLeninRickyОценок пока нет
- Cell Wall Inhibitors - Pharmacology 3 - Frank SsengoobaДокумент16 страницCell Wall Inhibitors - Pharmacology 3 - Frank SsengoobaVhugala AudreyОценок пока нет
- Urinary Tract Infection, Complicated (UTI) - Johns Hopkins ABX GuideДокумент5 страницUrinary Tract Infection, Complicated (UTI) - Johns Hopkins ABX GuideLaoMed plusОценок пока нет
- Introduction To Beta Lactam AntibioticsДокумент31 страницаIntroduction To Beta Lactam AntibioticsVishaal BhatОценок пока нет
- Print Antibiotics ReviewДокумент6 страницPrint Antibiotics ReviewtiuwangОценок пока нет
- AntibioticsДокумент11 страницAntibioticsSeshu Kelam100% (2)
- MCQ AnaesthesiaДокумент15 страницMCQ AnaesthesiaProf-Ashraf Emara100% (2)
- AAOS Anatomy 2008Документ63 страницыAAOS Anatomy 2008Dr-fadi AlkhasawnehОценок пока нет
- Restoration of The Worn Dentition. Part 2Документ7 страницRestoration of The Worn Dentition. Part 2Isharajini Prasadika Subhashni GamageОценок пока нет
- Classification of AntibioticsДокумент4 страницыClassification of AntibioticsNico AvellanaОценок пока нет
- Biological Considerations For Maxillary ImpressionsДокумент18 страницBiological Considerations For Maxillary ImpressionsVikas AggarwalОценок пока нет
- Step 1 DrugsДокумент46 страницStep 1 DrugsZebram ZeeОценок пока нет
- Code Blue Drill ResourceДокумент4 страницыCode Blue Drill ResourceZul Fahmi Prima100% (1)
- Helicobacter PyloriДокумент42 страницыHelicobacter Pyloritummalapalli venkateswara raoОценок пока нет
- Antibiotics PDFДокумент8 страницAntibiotics PDFSarah JaneОценок пока нет
- AntibioticsДокумент4 страницыAntibioticsVladimir GurjanovОценок пока нет
- Chemotherapy: BY Professor Dr. Ahmed KhalilДокумент29 страницChemotherapy: BY Professor Dr. Ahmed KhalilSAYED ZAKIОценок пока нет
- AntibacterialsДокумент8 страницAntibacterialslisalynnleeОценок пока нет
- Aminoglycoside & CephalosporinsДокумент30 страницAminoglycoside & CephalosporinskrishnakumarОценок пока нет
- CefaclorДокумент3 страницыCefaclorAyah PaasaОценок пока нет
- OS217 LEC06 Rational Antibiotic UseДокумент6 страницOS217 LEC06 Rational Antibiotic Usegenerics54321Оценок пока нет
- Clinical Pharmacology - Rationale Behind Antibiotics PrescriptionДокумент12 страницClinical Pharmacology - Rationale Behind Antibiotics PrescriptionhalesОценок пока нет
- AntibioticsДокумент6 страницAntibioticsCyrus100% (1)
- Quinolones KSRPAIДокумент36 страницQuinolones KSRPAIwolverine12309Оценок пока нет
- Pharmacotherapy of ENT InfectionsДокумент86 страницPharmacotherapy of ENT InfectionsHoque Mohammed Newaz ShorifulОценок пока нет
- Antibiotic 1 PDFДокумент2 страницыAntibiotic 1 PDFmicheal1960Оценок пока нет
- Pharmacology II 352 CДокумент15 страницPharmacology II 352 CMustafa SaßerОценок пока нет
- Antibacterial SДокумент40 страницAntibacterial SAiman SohailОценок пока нет
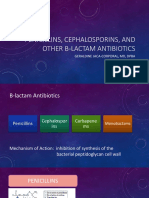
- Pencillins, Cephalosporins and Other B-Lactam AntibioticsДокумент45 страницPencillins, Cephalosporins and Other B-Lactam AntibioticsvishwaОценок пока нет
- Tratament PneumonieДокумент32 страницыTratament PneumonieSerban Elena100% (1)
- Pharma-URO-CYCLIC LIPOEPETIDES (Vancomycin)Документ6 страницPharma-URO-CYCLIC LIPOEPETIDES (Vancomycin)Hussein AlhaddadОценок пока нет
- Antibiotics ReviewДокумент4 страницыAntibiotics ReviewMariz OteroОценок пока нет
- Anti Infection AgentsДокумент18 страницAnti Infection AgentsRawabi SalehОценок пока нет
- Dr. Lilian - Beta Lactam AntibiotikДокумент35 страницDr. Lilian - Beta Lactam AntibiotikMeidikaWulandariОценок пока нет
- Sulphonamides & Co - Trimoxazole BamsДокумент46 страницSulphonamides & Co - Trimoxazole BamsKasturiRangan SrivatsaОценок пока нет
- Monobactams & CarbapenemsДокумент41 страницаMonobactams & CarbapenemsHussein AlhaddadОценок пока нет
- Antibiotics and Antibacterial DrugsДокумент69 страницAntibiotics and Antibacterial DrugsJames PerianayagamОценок пока нет
- AntibioticsДокумент56 страницAntibioticstintinОценок пока нет
- Drug Treatment of Pulmonary Tuberculosis: 4 Medical Year PharmacologyДокумент30 страницDrug Treatment of Pulmonary Tuberculosis: 4 Medical Year PharmacologyRuchi KholiyaОценок пока нет
- COTRIMOXAZOLE +FQsДокумент62 страницыCOTRIMOXAZOLE +FQsHussein AlhaddadОценок пока нет
- Antibiotics F MCP 1Документ37 страницAntibiotics F MCP 1Mohamed ElraiyОценок пока нет
- Anti Microbial NotesДокумент10 страницAnti Microbial NotesMohammed Faisal UddinОценок пока нет
- Profort VialДокумент8 страницProfort Vialelcapitano vegetaОценок пока нет
- ANTELMINTIKДокумент44 страницыANTELMINTIKnovi_linggaОценок пока нет
- Nursing 3703 Pharmacology: Antimicrobials by Linda SelfДокумент78 страницNursing 3703 Pharmacology: Antimicrobials by Linda Selfdon yenОценок пока нет
- Penicillins: 6-Amino Pencillanic Acid (6-APA)Документ14 страницPenicillins: 6-Amino Pencillanic Acid (6-APA)ThileepОценок пока нет
- Drugs I N Der Mato Lo GyДокумент85 страницDrugs I N Der Mato Lo GySilviuОценок пока нет
- The Kidney!) : Penicillin V Penicillin GДокумент10 страницThe Kidney!) : Penicillin V Penicillin GUsm LeeОценок пока нет
- 2 Beta Lactum 2020Документ25 страниц2 Beta Lactum 2020Sparks Francis EzikaОценок пока нет
- Infectious DiseaseДокумент31 страницаInfectious DiseasemirunahorgaОценок пока нет
- Pharma URO AminoglycosidesДокумент8 страницPharma URO AminoglycosidesHussein AlhaddadОценок пока нет
- Lecture 31 Beta-Lactam (Table)Документ5 страницLecture 31 Beta-Lactam (Table)Stephie E.Оценок пока нет
- Cirilo Albert Hicban RN, RM LecturerДокумент50 страницCirilo Albert Hicban RN, RM Lecturerrongan008Оценок пока нет
- Antibiotic AntimicrobialДокумент52 страницыAntibiotic Antimicrobialomereladil100% (1)
- Aminoglycosides AntibioticsДокумент2 страницыAminoglycosides AntibioticsHlaSoe WinОценок пока нет
- September 2015 Ophthalmic PearlsДокумент3 страницыSeptember 2015 Ophthalmic PearlsLouis WakumОценок пока нет
- Danielle Armour Resume 2017Документ1 страницаDanielle Armour Resume 2017daniellearmour24Оценок пока нет
- Case Study FIXДокумент66 страницCase Study FIXPatrick Kelvian100% (1)
- 940837-000001 LMA-Protector Factsheet 1604Документ2 страницы940837-000001 LMA-Protector Factsheet 1604nanang criztaОценок пока нет
- Final SPR 10 Student SyllabusДокумент61 страницаFinal SPR 10 Student SyllabusHilux23Оценок пока нет
- Adrenergic Receptor AntagonistsДокумент9 страницAdrenergic Receptor AntagonistsPatterson MachariaОценок пока нет
- Improving The Quality of Pain Management Through Measurement and ActionДокумент115 страницImproving The Quality of Pain Management Through Measurement and ActionNational Pharmaceutical Council100% (1)
- English Final ExamsДокумент2 страницыEnglish Final ExamsOgyKaikuzenОценок пока нет
- Hospital Disaster Management Guidelines: Directorate of Health Services, KeralaДокумент56 страницHospital Disaster Management Guidelines: Directorate of Health Services, KeralaPrasetya PerwiraОценок пока нет
- ArticleДокумент9 страницArticlernvisОценок пока нет
- K Burns Qualitative Research PosterДокумент1 страницаK Burns Qualitative Research Posterapi-257576036Оценок пока нет
- Madeleine Leininger and The Transcultural Theory of NursingДокумент8 страницMadeleine Leininger and The Transcultural Theory of NursingTommy PangandahengОценок пока нет
- YASASII - Nursing ManualДокумент20 страницYASASII - Nursing ManualSalma Alsheikh AbdullahОценок пока нет
- Kala AzarДокумент37 страницKala AzarMamata ManandharОценок пока нет
- Ranitidine 50mg - 2ml Solution For Injection and Infusion - (EMC) Print FriendlyДокумент6 страницRanitidine 50mg - 2ml Solution For Injection and Infusion - (EMC) Print FriendlyDewi Wara ShintaОценок пока нет
- NCP (Fatigue)Документ3 страницыNCP (Fatigue)Edrick SilvaОценок пока нет
- Nursing InformaticsДокумент16 страницNursing InformaticsSherina W. Edding100% (2)
- Agencies WebsitesДокумент4 страницыAgencies WebsitesWWMTОценок пока нет
- United Biotech WorldДокумент9 страницUnited Biotech Worldswtyneha33Оценок пока нет