HB 3309-4 (LC 2931) 5/22/13 (LHF/ps)
PROPOSED AMENDMENTS TO HOUSE BILL 3309
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22
On page 1 of the printed bill, delete lines 5 and 6 and insert: SECTION 1. The Oregon Health Authority shall conduct a pilot project in Marion and Polk Counties. In the pilot project: (1) The board of directors of a coordinated care organization that serves members residing in Marion County or Polk County may petition. In line 22, delete the period and insert or upon the termination of the pilot project, whichever occurs first. (5) A board member who represents a county government may not be removed under the pilot project. SECTION 2. No later than 12 months after the effective date of this 2013 Act, the Oregon Health Authority shall report to the House Interim Committee on Health Care in the manner prescribed by ORS 192.245: (1) The results of the pilot project; (2) Recommendations for legislative changes to the pilot project; and (3) Recommendations for expanding the pilot project statewide.. On page 3, line 30, delete 2 and insert 1. In line 31, delete board of directors and insert governing body. In line 33, delete board and insert governing body. On page 5, line 16, delete 2 and insert 1. On page 9, after line 42, insert:
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30
SECTION 8. ORS 414.625, as amended by section 3 of this 2013 Act, is amended to read: 414.625. (1) The Oregon Health Authority shall adopt by rule the qualification criteria and requirements for the certification of a coordinated care organization and shall integrate the criteria and requirements into each contract with a coordinated care organization. Coordinated care organizations may be local, community-based organizations or statewide organizations with community-based participation in governance or any combination of the two. Coordinated care organizations may contract with counties or with other public or private entities to provide services to members. The authority may not contract with only one statewide organization. A coordinated care organization may be a single corporate structure or a network of providers organized through contractual relationships. The criteria adopted by the authority under this section must include, but are not limited to, the coordinated care organizations demonstrated experience and capacity for: (a) Managing financial risk and establishing financial reserves. (b) Meeting the following minimum financial requirements: (A) Maintaining restricted reserves of $250,000 plus an amount equal to 50 percent of the coordinated care organizations total actual or projected liabilities above $250,000. (B) Maintaining a net worth in an amount equal to at least five percent of the average combined revenue in the prior two quarters of the participating health care entities. (c) Operating within a fixed global budget. (d) Developing and implementing alternative payment methodologies that are based on health care quality and improved health outcomes. (e) Coordinating the delivery of physical health care, mental health and chemical dependency services, oral health care and covered long-term care services.
HB 3309-4 5/22/13 Proposed Amendments to HB 3309
Page 2
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30
(f) Engaging community members and health care providers in improving the health of the community and addressing regional, cultural, socioeconomic and racial disparities in health care that exist among the coordinated care organizations members and in the coordinated care organizations community. (2) In addition to the criteria specified in subsection (1) of this section, the authority must adopt by rule certification requirements for coordinated care organizations contracting with the authority so that: (a) Each member of the coordinated care organization receives integrated person centered care and services designed to provide choice, independence and dignity. (b) Each member has a consistent and stable relationship with a care team that is responsible for comprehensive care management and service delivery. (c) The supportive and therapeutic needs of each member are addressed in a holistic fashion, using patient centered primary care homes or other models that support patient centered primary care and individualized care plans to the extent feasible. (d) Members receive comprehensive transitional care, including appropriate follow-up, when entering and leaving an acute care facility or a long term care setting. (e) Members receive assistance in navigating the health care delivery system and in accessing community and social support services and statewide resources, including through the use of certified health care interpreters, as defined in ORS 413.550, community health workers and personal health navigators who meet competency standards established by the authority under ORS 414.665 or who are certified by the Home Care Commission under ORS 410.604. (f) Services and supports are geographically located as close to where members reside as possible and are, if available, offered in nontraditional
HB 3309-4 5/22/13 Proposed Amendments to HB 3309
Page 3
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30
settings that are accessible to families, diverse communities and underserved populations. (g) Each coordinated care organization uses health information technology to link services and care providers across the continuum of care to the greatest extent practicable and if financially viable. (h) Each coordinated care organization complies with the safeguards for members described in ORS 414.635. (i) Each coordinated care organization convenes a community advisory council that meets the criteria specified in section 13, chapter 8, Oregon Laws 2012. (j) Each coordinated care organization prioritizes working with members who have high health care needs, multiple chronic conditions, mental illness or chemical dependency and involves those members in accessing and managing appropriate preventive, health, remedial and supportive care and services to reduce the use of avoidable emergency room visits and hospital admissions. (k) Members have a choice of providers within the coordinated care organizations network and that providers participating in a coordinated care organization: (A) Work together to develop best practices for care and service delivery to reduce waste and improve the health and well-being of members. (B) Are educated about the integrated approach and how to access and communicate within the integrated system about a patients treatment plan and health history. (C) Emphasize prevention, healthy lifestyle choices, evidence-based practices, shared decision-making and communication. (D) Are permitted to participate in the networks of multiple coordinated care organizations. (E) Include providers of specialty care. (F) Are selected by coordinated care organizations using universal ap-
HB 3309-4 5/22/13 Proposed Amendments to HB 3309
Page 4
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30
plication and credentialing procedures, objective quality information and are removed if the providers fail to meet objective quality standards. (G) Work together to develop best practices for culturally appropriate care and service delivery to reduce waste, reduce health disparities and improve the health and well-being of members. (L) Each coordinated care organization reports on outcome and quality measures adopted under ORS 414.638 and participates in the health care data reporting system established in ORS 442.464 and 442.466. (m) Each coordinated care organization uses best practices in the management of finances, contracts, claims processing, payment functions and provider networks. (n) Each coordinated care organization participates in the learning collaborative described in ORS 442.210 (3). (o) [ Except as provided in section 1 of this 2013 Act,] Each coordinated care organization has a governing body that includes: (A) Individuals representing the health care entities that share in the financial risk of the organization who must constitute a majority of the governing body; (B) Individuals representing the major components of the health care delivery system; (C) At least two health care providers in active practice, including: (i) A physician licensed under ORS chapter 677 or a nurse practitioner certified under ORS 678.375, whose area of practice is primary care; and (ii) A mental health or chemical dependency treatment provider; (D) At least two members from the community at large, to ensure that the organizations decision-making is consistent with the values of the members and the community; and (E) At least one member of the community advisory council. (3) The authority shall consider the participation of area agencies and other nonprofit agencies in the configuration of coordinated care organiza-
HB 3309-4 5/22/13 Proposed Amendments to HB 3309
Page 5
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30
tions. (4) In selecting one or more coordinated care organizations to serve a geographic area, the authority shall: (a) For members and potential members, optimize access to care and choice of providers; (b) For providers, optimize choice in contracting with coordinated care organizations; and (c) Allow more than one coordinated care organization to serve the geographic area if necessary to optimize access and choice under this subsection. (5) On or before July 1, 2014, each coordinated care organization must have a formal contractual relationship with any dental care organization that serves members of the coordinated care organization in the area where they reside. SECTION 9. ORS 414.635, as amended by section 9, chapter 602, Oregon Laws 2011, and section 5, chapter 8, Oregon Laws 2012, and section 4 of this 2013 Act, is amended to read: 414.635. (1) The Oregon Health Authority shall adopt by rule safeguards for members enrolled in coordinated care organizations that protect against underutilization of services and inappropriate denials of services. In addition to any other consumer rights and responsibilities established by law, each member: (a) Must be encouraged to be an active partner in directing the members health care and services and not a passive recipient of care. (b) Must be educated about the coordinated care approach being used in the community and how to navigate the coordinated health care system. (c) Must have access to advocates, including qualified peer wellness specialists where appropriate, personal health navigators, and qualified community health workers who are part of the members care team to provide assistance that is culturally and linguistically appropriate to the
HB 3309-4 5/22/13 Proposed Amendments to HB 3309
Page 6
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30
members need to access appropriate services and participate in processes affecting the members care and services. (d) Shall be encouraged within all aspects of the integrated and coordinated health care delivery system to use wellness and prevention resources and to make healthy lifestyle choices. (e) Shall be encouraged to work with the members care team, including providers and community resources appropriate to the members needs as a whole person. (2) The authority shall establish and maintain an enrollment process for individuals who are dually eligible for Medicare and Medicaid that promotes continuity of care and that allows the member to disenroll from a coordinated care organization that fails to promptly provide adequate services and: (a) To enroll in another coordinated care organization of the members choice; or (b) If another organization is not available, to receive Medicare-covered services on a fee-for-service basis. (3) Members and their providers and coordinated care organizations have the right to appeal decisions about care and services through the authority in an expedited manner and in accordance with the contested case procedures in ORS chapter 183. (4) A health care entity may not unreasonably refuse to contract with an organization seeking to form a coordinated care organization if the participation of the entity is necessary for the organization to qualify as a coordinated care organization. (5) A health care entity may refuse to contract with a coordinated care organization if the reimbursement established for a service provided by the entity under the contract is below the reasonable cost to the entity for providing the service. (6) A health care entity that unreasonably refuses to contract with a coordinated care organization may not receive fee-for-service reimbursement
HB 3309-4 5/22/13 Proposed Amendments to HB 3309
Page 7
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26
from the authority for services that are available through a coordinated care organization either directly or by contract. (7) The authority shall adopt by rule a process for resolving disputes involving an entitys refusal to contract with a coordinated care organization under subsections (4) and (5) of this section. The process must include the use of an independent third party arbitrator. (8) A coordinated care organization may not unreasonably refuse to contract with a licensed health care provider. (9) The authority shall: (a) Monitor and enforce consumer rights and protections within the Oregon Integrated and Coordinated Health Care Delivery System and ensure a consistent response to complaints of violations of consumer rights or protections. (b) Monitor and report on the statewide health care expenditures and recommend actions appropriate and necessary to contain the growth in health care costs incurred by all sectors of the system. (c) Decertify a coordinated care organization that[ : ] [ (A) ] substantially fails to comply with rules adopted pursuant to ORS 414.625 or this section[; or] [ (B) Fails to comply with section 1 (3) of this 2013 Act]. SECTION 10. The amendments to ORS 414.625 and 414.635 by sections 8 and 9 of this 2013 Act become operative January 2, 2018. SECTION 11. Sections 1 and 2 of this 2013 Act are repealed January 2, 2018.. In line 43, delete 8 and insert 12.
HB 3309-4 5/22/13 Proposed Amendments to HB 3309
Page 8
Вам также может понравиться
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Resource List For Trauma Responses: Grounding Breathing Exercises To Take You Out of "Fight/Flight" ModeДокумент3 страницыResource List For Trauma Responses: Grounding Breathing Exercises To Take You Out of "Fight/Flight" ModeStatesman JournalОценок пока нет
- Automation in Pharmacy PDFДокумент39 страницAutomation in Pharmacy PDFanthonyОценок пока нет
- Bronchopneumonia Care PlanДокумент6 страницBronchopneumonia Care PlanAbhijit Soundade0% (1)
- Roads and Trails of Cascade HeadДокумент1 страницаRoads and Trails of Cascade HeadStatesman JournalОценок пока нет
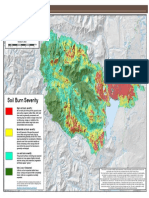
- Cedar Creek Fire Soil Burn SeverityДокумент1 страницаCedar Creek Fire Soil Burn SeverityStatesman JournalОценок пока нет
- Letter To Judge Hernandez From Rural Oregon LawmakersДокумент4 страницыLetter To Judge Hernandez From Rural Oregon LawmakersStatesman JournalОценок пока нет
- Complaint Summary Memo To Superintendent Re 8-9 BD Meeting - CB 9-14-22Документ4 страницыComplaint Summary Memo To Superintendent Re 8-9 BD Meeting - CB 9-14-22Statesman JournalОценок пока нет
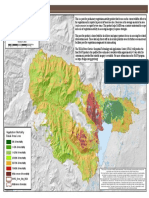
- Cedar Creek Vegitation Burn SeverityДокумент1 страницаCedar Creek Vegitation Burn SeverityStatesman JournalОценок пока нет
- Mount Hood National Forest Map of Closed and Open RoadsДокумент1 страницаMount Hood National Forest Map of Closed and Open RoadsStatesman JournalОценок пока нет
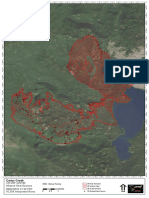
- Cedar Creek Fire Sept. 3Документ1 страницаCedar Creek Fire Sept. 3Statesman JournalОценок пока нет
- Revised Closure of The Beachie/Lionshead FiresДокумент4 страницыRevised Closure of The Beachie/Lionshead FiresStatesman JournalОценок пока нет
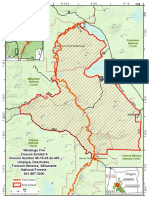
- Windigo Fire ClosureДокумент1 страницаWindigo Fire ClosureStatesman JournalОценок пока нет
- School Board Zones Map 2021Документ1 страницаSchool Board Zones Map 2021Statesman JournalОценок пока нет
- Matthieu Lake Map and CampsitesДокумент1 страницаMatthieu Lake Map and CampsitesStatesman JournalОценок пока нет
- Proclamation Parent & Guardian Engagement in Education 1-11-22 Final, SignedДокумент1 страницаProclamation Parent & Guardian Engagement in Education 1-11-22 Final, SignedStatesman JournalОценок пока нет
- Op Ed - Anthony MedinaДокумент2 страницыOp Ed - Anthony MedinaStatesman JournalОценок пока нет
- Crib Midget Day Care Emergency Order of SuspensionДокумент6 страницCrib Midget Day Care Emergency Order of SuspensionStatesman JournalОценок пока нет
- Salem-Keizer Parent and Guardian Engagement in Education Month ProclamationДокумент1 страницаSalem-Keizer Parent and Guardian Engagement in Education Month ProclamationStatesman JournalОценок пока нет
- LGBTQ Proclaimation 2022Документ1 страницаLGBTQ Proclaimation 2022Statesman JournalОценок пока нет
- Salem-Keizer Discipline Data Dec. 2021Документ13 страницSalem-Keizer Discipline Data Dec. 2021Statesman JournalОценок пока нет
- SIA Report 2022 - 21Документ10 страницSIA Report 2022 - 21Statesman JournalОценок пока нет
- Oregon Annual Report Card 2020-21Документ71 страницаOregon Annual Report Card 2020-21Statesman JournalОценок пока нет
- 2021 Ironman 70.3 Oregon Traffic ImpactДокумент2 страницы2021 Ironman 70.3 Oregon Traffic ImpactStatesman JournalОценок пока нет
- Statement From Marion County Medical Examiner's Office On Heat-Related DeathsДокумент1 страницаStatement From Marion County Medical Examiner's Office On Heat-Related DeathsStatesman JournalОценок пока нет
- Gcab - Personal Electronic Devices and Social Media - StaffДокумент2 страницыGcab - Personal Electronic Devices and Social Media - StaffStatesman JournalОценок пока нет
- Zone Resolution PDFДокумент2 страницыZone Resolution PDFStatesman JournalОценок пока нет
- City of Salem Photo Red Light Program 2021 Legislative ReportДокумент8 страницCity of Salem Photo Red Light Program 2021 Legislative ReportStatesman JournalОценок пока нет
- Schools, Safe Learners (RSSL) Guidance. We Have Established A Statewide Rapid Testing ProgramДокумент3 страницыSchools, Safe Learners (RSSL) Guidance. We Have Established A Statewide Rapid Testing ProgramStatesman Journal100% (1)
- SB Agenda 20210415 EnglishДокумент1 страницаSB Agenda 20210415 EnglishStatesman JournalОценок пока нет
- School Board Zone MapДокумент1 страницаSchool Board Zone MapStatesman JournalОценок пока нет
- Student Copy Conti - Intrapartal Week8Документ25 страницStudent Copy Conti - Intrapartal Week8Toyour EternityОценок пока нет
- Head Injury Lect 5Документ27 страницHead Injury Lect 5amber tariq100% (1)
- Irene Gee Regidor BSED-English Conditions of Developmental Delay 1. Mental RetardationДокумент3 страницыIrene Gee Regidor BSED-English Conditions of Developmental Delay 1. Mental RetardationAliana CabalunaОценок пока нет
- Figure 1. New Criteria For AKI Diagnosis Are Displayed. in Order To Diagnose AKIДокумент8 страницFigure 1. New Criteria For AKI Diagnosis Are Displayed. in Order To Diagnose AKIMayra Alejandra Prada SerranoОценок пока нет
- Crown & Bridge RemovalДокумент1 страницаCrown & Bridge RemovalCamilaОценок пока нет
- 2013 Observer - Applicant FormsДокумент11 страниц2013 Observer - Applicant FormsshengzhoumiОценок пока нет
- CBT For KidsДокумент34 страницыCBT For KidsJelena VisekrunaОценок пока нет
- Sleeping Habits Classroom Behaviour andДокумент10 страницSleeping Habits Classroom Behaviour andSamir SolimanОценок пока нет
- Assessment of Knowledge Attitude and Perception of Dental Students Towards Obesity in Kanpur CityДокумент6 страницAssessment of Knowledge Attitude and Perception of Dental Students Towards Obesity in Kanpur CityAdvanced Research PublicationsОценок пока нет
- Anthropometric ResultДокумент2 страницыAnthropometric ResultNaveed AhmedОценок пока нет
- Kernow LMC Newsletter - October 2019 Edition FINAL USE For WebsiteДокумент14 страницKernow LMC Newsletter - October 2019 Edition FINAL USE For WebsiteCornwall and Isles of Scilly LMCОценок пока нет
- UN Declaration of The Rights of The Child (1959)Документ2 страницыUN Declaration of The Rights of The Child (1959)bonalawОценок пока нет
- Pediatrics 2013 Kapadia E1488 96Документ11 страницPediatrics 2013 Kapadia E1488 96M Aprial DarmawanОценок пока нет
- EO-GA-32 Continued Response To COVID-19 IMAGE 10-07-2020Документ7 страницEO-GA-32 Continued Response To COVID-19 IMAGE 10-07-2020Jakob RodriguezОценок пока нет
- Normal Random Blood Sugar - Google SearchДокумент1 страницаNormal Random Blood Sugar - Google SearchmechОценок пока нет
- Product Brochure 2023-2024 en LRДокумент23 страницыProduct Brochure 2023-2024 en LRaf8009035Оценок пока нет
- Kriyakala AvastaДокумент13 страницKriyakala Avastakundagol100% (1)
- Asynchronous Activities IE 533Документ34 страницыAsynchronous Activities IE 533Ryanne TeñosoОценок пока нет
- Coronary Drug Eluting Stents Nonclinical and Clinical StudiesДокумент89 страницCoronary Drug Eluting Stents Nonclinical and Clinical Studiesdudde niranjanОценок пока нет
- Albumin Administration in The Acutely Ill: What Is New and Where Next?Документ10 страницAlbumin Administration in The Acutely Ill: What Is New and Where Next?Peter AgabaОценок пока нет
- Temy Dlya Napisania Esse V EGE Po Angliyskomu YazykuДокумент7 страницTemy Dlya Napisania Esse V EGE Po Angliyskomu YazykuElena StepanovaОценок пока нет
- Differential Diagnosis of Cervical CancerДокумент8 страницDifferential Diagnosis of Cervical Cancerrey martinoОценок пока нет
- Introduction of Air Ambulance Services in IndiaДокумент5 страницIntroduction of Air Ambulance Services in Indiaprithvinatarajan100% (1)
- CSHP TEMPLATE (1) - NewДокумент14 страницCSHP TEMPLATE (1) - NewLucky JavellanaОценок пока нет
- Abdominal Aortic Aneurysm: Gilbert R. Upchurch, JR., M.D., and Timothy A. Schaub, M.DДокумент7 страницAbdominal Aortic Aneurysm: Gilbert R. Upchurch, JR., M.D., and Timothy A. Schaub, M.DleesaОценок пока нет
- Anemia ProjectДокумент33 страницыAnemia ProjectNilesh BagalОценок пока нет
- Systemic Response To InjuryДокумент15 страницSystemic Response To InjuryJohnVincentPagaddu100% (1)
- Basic Nutrition: Ma - Aileen C. Carating RNDДокумент13 страницBasic Nutrition: Ma - Aileen C. Carating RNDspaspanОценок пока нет