Вам также может понравиться
- Borang Permohonan Pegawai Perubatan Kontrak (Warganegara) Di Kementerian Kesihatan MalaysiaДокумент15 страницBorang Permohonan Pegawai Perubatan Kontrak (Warganegara) Di Kementerian Kesihatan MalaysiaNuruldina AliaОценок пока нет
- Application Form For Contract Medical Officer (Non - Citizens) PDFДокумент19 страницApplication Form For Contract Medical Officer (Non - Citizens) PDFHafiz IbrahimОценок пока нет
- Application Form (HO) - 2013Документ15 страницApplication Form (HO) - 2013Maza LufiasОценок пока нет
- Provisional Registration Sop July 2 PDFДокумент8 страницProvisional Registration Sop July 2 PDFain julaikhaaОценок пока нет
- Provisional Registration - Guide & Forms PDFДокумент9 страницProvisional Registration - Guide & Forms PDFKelvinTeoОценок пока нет
- Malaysian Medical Council Guideline & Application FormДокумент11 страницMalaysian Medical Council Guideline & Application FormFarhana AnmusОценок пока нет
- Annual Practicing Certificate (Apc) Guideline PDFДокумент4 страницыAnnual Practicing Certificate (Apc) Guideline PDFKhalid BipersОценок пока нет
- Application For Gainful Occupational PermitДокумент6 страницApplication For Gainful Occupational PermitangelobelvisoОценок пока нет
- Malaysian Medical Council Guidelines and Application Form For Provisional RegistrationДокумент5 страницMalaysian Medical Council Guidelines and Application Form For Provisional RegistrationaisyahxyzОценок пока нет
- Annual Practicing Certificate (Apc)Документ6 страницAnnual Practicing Certificate (Apc)Husain R Saeed100% (1)
- 5.letter of Good StandingДокумент6 страниц5.letter of Good Standingkayzinhtaik100% (3)
- DataFlow Application PackДокумент8 страницDataFlow Application PackvaranasidineshОценок пока нет
- HCP Guidelines Licensure For All Professionals PDFДокумент9 страницHCP Guidelines Licensure For All Professionals PDFvinay kumarОценок пока нет
- DeclarationДокумент3 страницыDeclarationmoon oadОценок пока нет
- Sundargarh Recruitment 2013 For Paramedical PostДокумент8 страницSundargarh Recruitment 2013 For Paramedical PostmotilalprusethОценок пока нет
- Detailed Instructions For Candidates Attending Personality Test Board in Respect of Combined Medical Services Examination, 2017Документ2 страницыDetailed Instructions For Candidates Attending Personality Test Board in Respect of Combined Medical Services Examination, 2017Diwakesh C BОценок пока нет
- Andaman & Nicobar Union Territory Health MissionДокумент1 страницаAndaman & Nicobar Union Territory Health MissionombidasarОценок пока нет
- RN enДокумент30 страницRN enrsa_proctorОценок пока нет
- Dental Specialist ApplicationsДокумент7 страницDental Specialist ApplicationsanukeysОценок пока нет
- SRF Advertisement - 10-April-2023Документ4 страницыSRF Advertisement - 10-April-2023Jatin R RawalОценок пока нет
- Annual Practicing Certificate Guide Forms v2 LATEST 2Документ4 страницыAnnual Practicing Certificate Guide Forms v2 LATEST 2Aida Rosniza SufisiberОценок пока нет
- Cantonment General Hospital Delhi Cantonment Board Delhi Cantt. - 10 Engagement NoticeДокумент6 страницCantonment General Hospital Delhi Cantonment Board Delhi Cantt. - 10 Engagement NoticeKamal MakkarОценок пока нет
- Guideline and Application Form For Relaxation of Compulsory ServiceДокумент13 страницGuideline and Application Form For Relaxation of Compulsory ServiceUwais Al Qorni HashimahОценок пока нет
- F.No. 8-10/2010-Admn - II (A) Government of India O/o The Medical Superintendent Safdarjang Hospital & VMMC New Delhi-110029Документ2 страницыF.No. 8-10/2010-Admn - II (A) Government of India O/o The Medical Superintendent Safdarjang Hospital & VMMC New Delhi-110029pervinkumarОценок пока нет
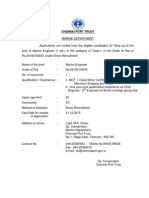
- Chennai Port TrustДокумент5 страницChennai Port TrustpothirajkalyanОценок пока нет
- New Midwifery Requirements: 1 Basic RequirementДокумент4 страницыNew Midwifery Requirements: 1 Basic RequirementJeanne Salvador CoronelОценок пока нет
- AIIMSsnДокумент5 страницAIIMSsnJeshiОценок пока нет
- PG Bulletin 2013Документ20 страницPG Bulletin 2013Rahat SalОценок пока нет
- Instruction To Candidates Updated 17-10-2012Документ6 страницInstruction To Candidates Updated 17-10-2012Mobin SafdarОценок пока нет
- Physical Therapy Resume SampleДокумент27 страницPhysical Therapy Resume SampleDavid MancaoОценок пока нет
- Application Form: Mission Director UT Health MissionДокумент1 страницаApplication Form: Mission Director UT Health MissionKirankumar MutnaliОценок пока нет
- PMDC Reg FormДокумент2 страницыPMDC Reg Formhap hazardОценок пока нет
- DataFlow Application PackДокумент8 страницDataFlow Application PackMichelle TolentinoОценок пока нет
- NBE Recruitment 2021Документ16 страницNBE Recruitment 2021Divyansh SethОценок пока нет
- Mds ProspectusДокумент39 страницMds ProspectusSaravanan KanagavelОценок пока нет
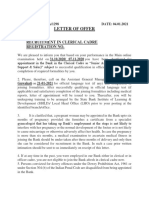
- Letter of Offer: Recruitment in Clerical Cadre Registration NoДокумент6 страницLetter of Offer: Recruitment in Clerical Cadre Registration NoDevdutt MishraОценок пока нет
- Notification Office of The Commissioner of The Health and Family Welfare AP Civil Asst Surgeon PostsДокумент8 страницNotification Office of The Commissioner of The Health and Family Welfare AP Civil Asst Surgeon PostsJeshiОценок пока нет
- Medical Council of India: Application Form For Migration From One Medical College To Another Medical College in IndiaДокумент8 страницMedical Council of India: Application Form For Migration From One Medical College To Another Medical College in IndiaHumble LuxuriantОценок пока нет
- Application For Registration Form August 3Документ7 страницApplication For Registration Form August 3alaaelbatawyОценок пока нет
- Notification GTB Hospital Staff Nurse PharmacistДокумент6 страницNotification GTB Hospital Staff Nurse PharmacistRuthvik Reddy0% (1)
- Application For Assessment of Training: Required Form For Entry To The MRCOG Part 3 Membership Exam Personal InformationДокумент4 страницыApplication For Assessment of Training: Required Form For Entry To The MRCOG Part 3 Membership Exam Personal InformationMd ZhidОценок пока нет
- Application Form Thiruvalluvar University Non Teaching PostsДокумент6 страницApplication Form Thiruvalluvar University Non Teaching PostsMagesssОценок пока нет
- BNS Requirements EligibilityДокумент6 страницBNS Requirements EligibilityPaul BronОценок пока нет
- Form-I: Affix Passport Size PhotographДокумент3 страницыForm-I: Affix Passport Size Photographዘረአዳም ዘመንቆረርОценок пока нет
- Requirements For GPsДокумент4 страницыRequirements For GPsSam VuppalОценок пока нет
- Certificate of Good StandingsДокумент5 страницCertificate of Good Standingsdigantpathak0% (1)
- Form VIII+Duplicate+Registration+CertificateДокумент2 страницыForm VIII+Duplicate+Registration+CertificatefaisalbasraОценок пока нет
- Temporary Registration Non-ScheduleДокумент7 страницTemporary Registration Non-Schedulevicky611Оценок пока нет
- Application Form For Obtaining A Certificate of Good StandingДокумент2 страницыApplication Form For Obtaining A Certificate of Good Standingshraddha5jОценок пока нет
- General Information On The Career Service Examinations Professional and SubДокумент4 страницыGeneral Information On The Career Service Examinations Professional and SubChristopher L. CalagosОценок пока нет
- Requirements For GPs enДокумент4 страницыRequirements For GPs enNazОценок пока нет
- AIIMS RishikeshДокумент5 страницAIIMS RishikeshKrishnaveni MurugeshОценок пока нет
- Qualification Recognition ManualДокумент16 страницQualification Recognition Manualannapanna1Оценок пока нет
- Inpatient Obstetric Nurse Exam Prep 2020-2021: A New Study Guide for Certification Including 300 Test Questions and Answers with Full Explanations (RNC-OB)От EverandInpatient Obstetric Nurse Exam Prep 2020-2021: A New Study Guide for Certification Including 300 Test Questions and Answers with Full Explanations (RNC-OB)Оценок пока нет
- Cross-Training: The Medical Assistant WorkbookОт EverandCross-Training: The Medical Assistant WorkbookОценок пока нет
- Study Permit: Working While Studying, Exemptions & How to ApplyОт EverandStudy Permit: Working While Studying, Exemptions & How to ApplyОценок пока нет
- California Notary Public Study Guide with 7 Practice Exams: 280 Practice Questions and 100+ Bonus Questions IncludedОт EverandCalifornia Notary Public Study Guide with 7 Practice Exams: 280 Practice Questions and 100+ Bonus Questions IncludedОценок пока нет
- Frequently Asked Questions - HLM Takaful Tenang & HLM Takaful Tenang 50Документ3 страницыFrequently Asked Questions - HLM Takaful Tenang & HLM Takaful Tenang 50Hafiz IbrahimОценок пока нет
- Manulife Precious Gift Brochure - Full - 100322Документ32 страницыManulife Precious Gift Brochure - Full - 100322Hafiz IbrahimОценок пока нет
- 21C EmotionalIntelligenceДокумент25 страниц21C EmotionalIntelligenceVaibhav P ShahОценок пока нет
- Book1 1Документ1 страницаBook1 1Hafiz IbrahimОценок пока нет
- Credit/Debit Card Authorisation (Autopay) (Visa / Mastercard / Amex)Документ2 страницыCredit/Debit Card Authorisation (Autopay) (Visa / Mastercard / Amex)Hafiz IbrahimОценок пока нет
- Aqad-Authorisation ENGДокумент1 страницаAqad-Authorisation ENGHafiz IbrahimОценок пока нет
- SingleDisciplinary GrantApp ManualДокумент52 страницыSingleDisciplinary GrantApp ManualHafiz IbrahimОценок пока нет
- The Functions of The Skeletal System 3Документ8 страницThe Functions of The Skeletal System 3Hafiz IbrahimОценок пока нет
- eScienceFund UserManualДокумент59 страницeScienceFund UserManualHafiz IbrahimОценок пока нет
- SOP & Flowchart (Student)Документ3 страницыSOP & Flowchart (Student)apit9Оценок пока нет
- Notes and Formulae MathematicsДокумент9 страницNotes and Formulae MathematicsPurplesnow CongbeautyОценок пока нет
- Online Registration Guide For Research Mode: 1. Progress ReportДокумент2 страницыOnline Registration Guide For Research Mode: 1. Progress ReportHafiz IbrahimОценок пока нет
- SingleDisciplinary GrantApp ManualДокумент52 страницыSingleDisciplinary GrantApp ManualHafiz IbrahimОценок пока нет
- UniKl 171114Документ1 страницаUniKl 171114Hafiz IbrahimОценок пока нет
- Guidelines - Science FundДокумент27 страницGuidelines - Science FundzeyrieОценок пока нет
- Analysing Data Using SpssДокумент94 страницыAnalysing Data Using SpssSandeep Bhatt100% (1)
- Library Membership Form - StudentДокумент1 страницаLibrary Membership Form - Studentapit9Оценок пока нет
- Course Work and Mix-Mode Programme Offered For February Intake Academic Session 2013/2014Документ2 страницыCourse Work and Mix-Mode Programme Offered For February Intake Academic Session 2013/2014Hafiz IbrahimОценок пока нет
- CPG Management of StrokeДокумент51 страницаCPG Management of Strokeapalaginih0% (1)
- Graduate Assistant Scheme 001Документ6 страницGraduate Assistant Scheme 001Hafiz IbrahimОценок пока нет
- Pam P Let Nuklear UpdatedДокумент2 страницыPam P Let Nuklear UpdatedHafiz IbrahimОценок пока нет
- Diabetes Mellitus - Type 2 DiabetesДокумент11 страницDiabetes Mellitus - Type 2 DiabetesHafiz IbrahimОценок пока нет
- Registration Guideline CWMMДокумент3 страницыRegistration Guideline CWMMHafiz IbrahimОценок пока нет
- Wavesandsounds 111128101828 Phpapp01Документ34 страницыWavesandsounds 111128101828 Phpapp01Hafiz IbrahimОценок пока нет
- Modul 13 IntegrationДокумент16 страницModul 13 Integrationhasnitajb0% (1)
- A. Circle The Correct AnswersДокумент9 страницA. Circle The Correct AnswersRossly HamidОценок пока нет
- Senarai Kursus Yang Ditawarkan Bagi Program Mod Kerja Kursus Dan Mod Campuran Semester 1 2013-2014 BIДокумент5 страницSenarai Kursus Yang Ditawarkan Bagi Program Mod Kerja Kursus Dan Mod Campuran Semester 1 2013-2014 BIHafiz IbrahimОценок пока нет
- Matematik - Tingkatan 3Документ66 страницMatematik - Tingkatan 3Sekolah Portal95% (19)
- Final List of Handouts (Math Advanced 2022)Документ2 страницыFinal List of Handouts (Math Advanced 2022)Keennith NarcaОценок пока нет
- Test Question Tags en Answers PDFДокумент3 страницыTest Question Tags en Answers PDFpedropesaoОценок пока нет
- Language - Analysis Simple Present Third Person PDFДокумент2 страницыLanguage - Analysis Simple Present Third Person PDFsoniaalbertazziОценок пока нет
- An Evaluation of The Traditional Education System by Kevin BondelliДокумент7 страницAn Evaluation of The Traditional Education System by Kevin BondelliKevin Bondelli100% (19)
- The Actfast Anti-Choking TrainerДокумент3 страницыThe Actfast Anti-Choking TrainerForum PompieriiОценок пока нет
- Civil Engineering 2011 0Документ2 страницыCivil Engineering 2011 0Darah GardnerОценок пока нет
- Computer Science HSSC I Syllabus and Model Question Paper Fbise PDFДокумент31 страницаComputer Science HSSC I Syllabus and Model Question Paper Fbise PDFAttique ZaheerОценок пока нет
- Ib Cas FactsДокумент20 страницIb Cas Factsmjlane3Оценок пока нет
- Formative EvaluationДокумент8 страницFormative Evaluationapi-269739127Оценок пока нет
- The Informal System and Hidden CurriculumДокумент2 страницыThe Informal System and Hidden CurriculumAzul, John Eric D.Оценок пока нет
- BCom Hons - Fin PlanДокумент12 страницBCom Hons - Fin PlanFrancis MtamboОценок пока нет
- Cox News Volume 7 Issue 16Документ4 страницыCox News Volume 7 Issue 16David M. Cox ESОценок пока нет
- Cover PDFДокумент2 страницыCover PDFsujayraviОценок пока нет
- CHAPTER 4,5 and Preliminaries TemplateДокумент7 страницCHAPTER 4,5 and Preliminaries TemplateSean ChuaОценок пока нет
- Lesson Plan - Number 7Документ2 страницыLesson Plan - Number 7api-295500001100% (2)
- Syllabus Vs CurriculumДокумент9 страницSyllabus Vs CurriculumWjdan AlahreshОценок пока нет
- Pcdmis ProДокумент175 страницPcdmis ProKemalMalovcic100% (2)
- Cefr Lesson Planning ListeningДокумент2 страницыCefr Lesson Planning ListeningPat Ednonymous Patrick100% (1)
- CURRENT TRENDS ISSUES IN NURSING EDUCATION Nursing EducationДокумент41 страницаCURRENT TRENDS ISSUES IN NURSING EDUCATION Nursing EducationLIDIYA MOL P V100% (7)
- PLCs and Pneumatic SystemsДокумент5 страницPLCs and Pneumatic SystemsKazi Mehdi0% (2)
- Designing Rich Numeracy Tasks: The University of QueenslandДокумент9 страницDesigning Rich Numeracy Tasks: The University of QueenslanddannyОценок пока нет
- Result CommentsДокумент8 страницResult CommentsDare Arqam100% (2)
- Cde Mba Mca 2011Документ43 страницыCde Mba Mca 2011raman25Оценок пока нет
- Lesson 1.4 RubricДокумент1 страницаLesson 1.4 RubricJohnny FlashОценок пока нет
- Trainers Methodology Level 1: Orientation April 10, 2019Документ44 страницыTrainers Methodology Level 1: Orientation April 10, 2019Kent Francisco100% (2)
- Doctor of Education (Edd) : Major Courses (Choose Any 10) Elective Courses (Choose Any 5)Документ1 страницаDoctor of Education (Edd) : Major Courses (Choose Any 10) Elective Courses (Choose Any 5)Tawau NzmОценок пока нет
- Angela Halliday 2016 Ubd Unit PlanДокумент11 страницAngela Halliday 2016 Ubd Unit Planapi-325865277100% (2)
- Philip Callan: Student Leadership ExperienceДокумент2 страницыPhilip Callan: Student Leadership ExperiencePhil LouisОценок пока нет
- How To Work As A Doctor in MalaysiaДокумент20 страницHow To Work As A Doctor in Malaysiarobin khanОценок пока нет
- Gr. 11 Course OutlineДокумент2 страницыGr. 11 Course Outlinekevinv10Оценок пока нет