Вам также может понравиться
- Fast Facts: Hyperlipidemia: Bringing clarity to lipid managementОт EverandFast Facts: Hyperlipidemia: Bringing clarity to lipid managementОценок пока нет
- Cardiac Function Tests GuideДокумент35 страницCardiac Function Tests GuideChandana Padma Priya JuturОценок пока нет
- Laboratory Procedure ManualДокумент23 страницыLaboratory Procedure ManualIseth ISethОценок пока нет
- Lipid Disorders PathophysiologyДокумент72 страницыLipid Disorders PathophysiologyBlodin ZylfiuОценок пока нет
- Lipid Profile L - DeterminatinДокумент33 страницыLipid Profile L - DeterminatinaliОценок пока нет
- Estimate Cholesterol Levels GuideДокумент4 страницыEstimate Cholesterol Levels Guidehaseeb ShafaatОценок пока нет
- 4.investigations of Serum LipidsДокумент7 страниц4.investigations of Serum LipidsMV ProductionОценок пока нет
- Cardiac DiagnosticsДокумент97 страницCardiac DiagnosticsNaomi Anne Asunto100% (1)
- AtherosclerosisДокумент29 страницAtherosclerosisneeraj banaОценок пока нет
- Lipid ProfileДокумент23 страницыLipid Profilekyawswakyawswa100% (1)
- Lipids Case StudiesДокумент6 страницLipids Case Studiesgogo29% (7)
- LipidsДокумент13 страницLipidsalianaОценок пока нет
- BCMTMS Practice Exam Answers PDF 2023Документ61 страницаBCMTMS Practice Exam Answers PDF 2023TammyОценок пока нет
- Medical Nutrition Therapy in Cardiovascular DiseaseДокумент93 страницыMedical Nutrition Therapy in Cardiovascular DiseasesariОценок пока нет
- LDLC3Документ4 страницыLDLC3Michael HenzuОценок пока нет
- Lab ValuesДокумент68 страницLab ValuesJayr ValmoresОценок пока нет
- Cardiovascular Disease: Interpretation of Clinical DataДокумент39 страницCardiovascular Disease: Interpretation of Clinical DataSapta DenyОценок пока нет
- Summary of Normal Laboratory ValuesДокумент24 страницыSummary of Normal Laboratory ValuesMissy U. TorrechillaОценок пока нет
- How Drugs Affect Lipid MetabolismДокумент50 страницHow Drugs Affect Lipid MetabolismchiragcvpОценок пока нет
- Chapter 15Документ5 страницChapter 15florenzo100% (3)
- Lipid and LipoproteinsДокумент4 страницыLipid and LipoproteinsDIEGO RAFAEL ESPIRITUОценок пока нет
- Lipid Profile: HDL & LDL CholesterolДокумент6 страницLipid Profile: HDL & LDL CholesterolQasmОценок пока нет
- Understanding Cholesterol Levels and Risks: A Guide to Lipid ProfilesДокумент48 страницUnderstanding Cholesterol Levels and Risks: A Guide to Lipid ProfilesAnonymous o3Q3QXEОценок пока нет
- Laboratory and Diagnostic FindingsДокумент4 страницыLaboratory and Diagnostic FindingsCG Patron BamboОценок пока нет
- Cardiac Enzyme Analysis: Anika Dahal Lecturer MmihsДокумент40 страницCardiac Enzyme Analysis: Anika Dahal Lecturer Mmihsanika dahalОценок пока нет
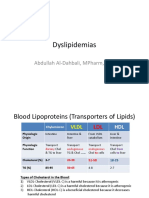
- Dyslipidemias: Abdullah Al-Dahbali, Mpharm, PHDДокумент15 страницDyslipidemias: Abdullah Al-Dahbali, Mpharm, PHDعزالدين الطيارОценок пока нет
- Lipoprotein Paper Academia ZaragedДокумент29 страницLipoprotein Paper Academia Zaragedpawovem755Оценок пока нет
- Inborn Errors of Lipid MetabolismДокумент41 страницаInborn Errors of Lipid MetabolismWalterОценок пока нет
- Normal Lab ValuesДокумент54 страницыNormal Lab ValuesShreyas Walvekar100% (3)
- Pharmacotherapy of Dyslipidemia by DR SarmaДокумент123 страницыPharmacotherapy of Dyslipidemia by DR Sarmamae2003Оценок пока нет
- Normal Lab Values Guide in 40 CharactersДокумент37 страницNormal Lab Values Guide in 40 CharactersKelly Camero ÜОценок пока нет
- Lipid ProfileДокумент20 страницLipid Profileمحمد هزاع الصبريОценок пока нет
- THYROID PROFILE REPORTДокумент7 страницTHYROID PROFILE REPORTSaujanyaSengarОценок пока нет
- Laboratory Values HandoutДокумент38 страницLaboratory Values HandoutSujia Nospiatdi50% (2)
- Estimation of Serum CholesterolДокумент44 страницыEstimation of Serum CholesterolHasan ShahriarОценок пока нет
- Normal Laboratory ValuesДокумент40 страницNormal Laboratory ValuesPrincess Nasima M. Usngan100% (1)
- Biochemistry "Lipids Test"Документ8 страницBiochemistry "Lipids Test"HEROОценок пока нет
- Cardiac Biomarkers: Cardiac Enzymes and BiomarkerДокумент21 страницаCardiac Biomarkers: Cardiac Enzymes and Biomarkeranamika sharmaОценок пока нет
- Case Study 2Документ2 страницыCase Study 2api-547174770100% (1)
- Analysis of Plasm LipoproteinДокумент10 страницAnalysis of Plasm LipoproteinWilson KhawОценок пока нет
- Cardiac Profile Tests GuideДокумент3 страницыCardiac Profile Tests GuideJim Varghese100% (1)
- Comparison of Two Homogeneous LDL-Cholesterol Assays Using Fresh Hypertriglyceridemic Serum and Quantitative Ultracentrifugation Fractions PDFДокумент10 страницComparison of Two Homogeneous LDL-Cholesterol Assays Using Fresh Hypertriglyceridemic Serum and Quantitative Ultracentrifugation Fractions PDFmagendi indra muktiОценок пока нет
- Diagnostic and Laboratory TestsДокумент13 страницDiagnostic and Laboratory TeststhexlndsyОценок пока нет
- Lipid Profile Disease and DiagnosisДокумент31 страницаLipid Profile Disease and DiagnosisGeetanjali JhaОценок пока нет
- Dyslipidemia overviewДокумент90 страницDyslipidemia overviewElena EllaОценок пока нет
- Lipid DisordersДокумент65 страницLipid DisordersNguyễn Minh Phương UyênОценок пока нет
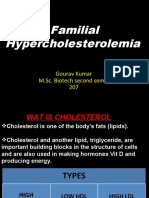
- Familial Hypercholesterolemia: Gourav Kumar M.Sc. Biotech Second Sem 2 207Документ43 страницыFamilial Hypercholesterolemia: Gourav Kumar M.Sc. Biotech Second Sem 2 207Gourav Kumar SinhaОценок пока нет
- Referat LP8-2E - CholesterolДокумент3 страницыReferat LP8-2E - CholesterolElena DalcaranОценок пока нет
- Triglycerides and VLDL: (Increased Ra Tio of Triglyceride To Apob)Документ20 страницTriglycerides and VLDL: (Increased Ra Tio of Triglyceride To Apob)Indah Pujiati DtОценок пока нет
- CK, LDH and Aldolase diagnostic significanceДокумент8 страницCK, LDH and Aldolase diagnostic significanceFrances del RosarioОценок пока нет
- 2008 Article BF02867401Документ8 страниц2008 Article BF02867401fachrurОценок пока нет
- VII. Laboratory Exams Name of Examination: Complete Blood Count DefinitionДокумент4 страницыVII. Laboratory Exams Name of Examination: Complete Blood Count DefinitionMark Ianne AngОценок пока нет
- DyslipidemiaДокумент44 страницыDyslipidemiaenri100% (1)
- Normal ValuesДокумент1 страницаNormal ValuesmimОценок пока нет
- Summary of Normal Laboratory ValuesДокумент37 страницSummary of Normal Laboratory ValuesHey it's FerdyОценок пока нет
- Nurseslabs Normal Lab Values 1.2 PDFДокумент5 страницNurseslabs Normal Lab Values 1.2 PDFPrincess BaciaОценок пока нет
- Measurement of serum lipids profile (Lipids Panel or Coronary Risk PanelДокумент26 страницMeasurement of serum lipids profile (Lipids Panel or Coronary Risk Panelزين العابدين محمد عويشОценок пока нет
- Cholesterol, Triglycerides, and Associated Lipoproteins - Clinical Methods - NCBI BookshelfДокумент30 страницCholesterol, Triglycerides, and Associated Lipoproteins - Clinical Methods - NCBI BookshelfNeha MasarkarОценок пока нет
- BBM Lipoprotein Metabolism Related DisordersДокумент26 страницBBM Lipoprotein Metabolism Related Disorderskaterina KarinaОценок пока нет
- Clinical Lab Result Interpretation-2 Dr. Bereket Molla TigabuДокумент41 страницаClinical Lab Result Interpretation-2 Dr. Bereket Molla Tigabuphoto copyhemnОценок пока нет
- 9Документ13 страниц9Osama BakheetОценок пока нет
- Practical Ielts Strategies 5 Test Practice Book 2015 An Insanely Dangerous Activities 5Документ3 страницыPractical Ielts Strategies 5 Test Practice Book 2015 An Insanely Dangerous Activities 5Osama Bakheet100% (1)
- Eua Biocerna Sars Euasum 0Документ7 страницEua Biocerna Sars Euasum 0Osama BakheetОценок пока нет
- 9Документ13 страниц9Osama BakheetОценок пока нет
- Mrsa in Latin AmericaДокумент12 страницMrsa in Latin AmericaOsama BakheetОценок пока нет
- Aborashad 2010 - Edit by Bosha11-4Документ96 страницAborashad 2010 - Edit by Bosha11-4Osama BakheetОценок пока нет
- Pembrolizumab Versus Docetaxel For Previously Treated, PD-L1-positive, Advanced Non-Small-Cell Lung Cancer (KEYNOTE-010) : A Randomised Controlled TrialДокумент12 страницPembrolizumab Versus Docetaxel For Previously Treated, PD-L1-positive, Advanced Non-Small-Cell Lung Cancer (KEYNOTE-010) : A Randomised Controlled TrialOSAMAОценок пока нет
- New England Journal Medicine: The ofДокумент12 страницNew England Journal Medicine: The ofOsama BakheetОценок пока нет
- 7Документ11 страниц7OSAMAОценок пока нет
- كيفية الحصول على شهادة البورد الامريكى للجمعية الأمريكية للكلينيكال باثولوجيДокумент11 страницكيفية الحصول على شهادة البورد الامريكى للجمعية الأمريكية للكلينيكال باثولوجيOsama BakheetОценок пока нет
- Lipids MetabolismДокумент19 страницLipids MetabolismOsama BakheetОценок пока нет
- Install Acrobatupd11021 First Install Acrobatupd11022 AfterДокумент1 страницаInstall Acrobatupd11021 First Install Acrobatupd11022 AfterOsama BakheetОценок пока нет
- 1Документ11 страниц1Osama BakheetОценок пока нет
- 182+سؤال+Документ27 страниц182+سؤال+Mohsen HaleemОценок пока нет
- كيفية الحصول على شهادة البورد الامريكى للجمعية الأمريكية للكلينيكال باثولوجيДокумент11 страницكيفية الحصول على شهادة البورد الامريكى للجمعية الأمريكية للكلينيكال باثولوجيOsama BakheetОценок пока нет
- كيفية الحصول على شهادة البورد الامريكى للجمعية الأمريكية للكلينيكال باثولوجيДокумент11 страницكيفية الحصول على شهادة البورد الامريكى للجمعية الأمريكية للكلينيكال باثولوجيOsama BakheetОценок пока нет
- Cross Matching Tests: Routine vs. Urgent Compatibility ProceduresДокумент2 страницыCross Matching Tests: Routine vs. Urgent Compatibility ProceduresOsama BakheetОценок пока нет
- 1grammar For IeltsДокумент71 страница1grammar For IeltsPaul Stato88% (8)
- Urinalysis SlidesДокумент10 страницUrinalysis SlidesOsama BakheetОценок пока нет
- Neisseria - Denise PDFДокумент2 страницыNeisseria - Denise PDFOsama BakheetОценок пока нет
- 2001 Pathology MCQДокумент11 страниц2001 Pathology MCQOsama Bakheet100% (1)
- Isolation of NeisseriaДокумент2 страницыIsolation of NeisseriaOsama Bakheet100% (1)
- Microbiology MR - VP Flashcards - QuizletДокумент4 страницыMicrobiology MR - VP Flashcards - QuizletOsama BakheetОценок пока нет
- MCB101 Introductory Microbiology LabДокумент8 страницMCB101 Introductory Microbiology LabOsama BakheetОценок пока нет
- MCQ in Microbiology Immunology Questions and Answers With ExplanationДокумент4 страницыMCQ in Microbiology Immunology Questions and Answers With ExplanationOsama Bakheet50% (2)
- BacteДокумент13 страницBacteAdriana GarciaОценок пока нет
- Molecular Biology BOC.Документ12 страницMolecular Biology BOC.Osama BakheetОценок пока нет
- User Manual Ed 6 July 09Документ34 страницыUser Manual Ed 6 July 09Osama BakheetОценок пока нет
- Analyzing Microbes Manual of Molecular Biology TechniquesДокумент367 страницAnalyzing Microbes Manual of Molecular Biology TechniquesOsama BakheetОценок пока нет
- StoolДокумент1 страницаStoolAhmed J AlhindaweОценок пока нет
- Statin Trial SummaryДокумент1 страницаStatin Trial SummaryThe Physician Assistant LifeОценок пока нет
- 13 Natural Ways to Treat HypothyroidismДокумент14 страниц13 Natural Ways to Treat HypothyroidismZelina KesavathparambilОценок пока нет
- Pharmacy ReviewerДокумент38 страницPharmacy Reviewerprincessrhenette67% (3)
- Miriam Stoppard-Trusted Advice PDFДокумент82 страницыMiriam Stoppard-Trusted Advice PDFoceanmist0101Оценок пока нет
- " Hypercholesterolemia: Pathophysiology and Therapeutics" "Hypercholesterolemia: Pathophysiology and Therapeutics"Документ7 страниц" Hypercholesterolemia: Pathophysiology and Therapeutics" "Hypercholesterolemia: Pathophysiology and Therapeutics"kookiescreamОценок пока нет
- Disease of Blood VesselsДокумент5 страницDisease of Blood VesselsKeshant SamarooОценок пока нет
- Virgin Coconut OilДокумент3 страницыVirgin Coconut OilEd CasasОценок пока нет
- Hypercholesterolemia PDFДокумент7 страницHypercholesterolemia PDFkookiescreamОценок пока нет
- Lindgarde 2000Документ10 страницLindgarde 2000fachry albabОценок пока нет
- New Approach For CV Risk Management (Prof. DR - Dr. Djanggan Sargowo, SPPD, SPJP (K) )Документ56 страницNew Approach For CV Risk Management (Prof. DR - Dr. Djanggan Sargowo, SPPD, SPJP (K) )Yulia SumarnaОценок пока нет
- Merck Form 10-kДокумент208 страницMerck Form 10-kKerine ChunОценок пока нет
- Opposing ViewsДокумент10 страницOpposing ViewsCarla ReddenОценок пока нет
- The Prevention of SchizophreniaДокумент6 страницThe Prevention of SchizophreniaMale BajoОценок пока нет
- Review Article Opuntia SPP.: Characterization and Benefits in Chronic DiseasesДокумент18 страницReview Article Opuntia SPP.: Characterization and Benefits in Chronic DiseasesVale PicoОценок пока нет
- Pitavastatin (Livalo®) : National Drug Monograph January 2012Документ18 страницPitavastatin (Livalo®) : National Drug Monograph January 2012anishОценок пока нет
- Media Medika IndonesianaДокумент8 страницMedia Medika IndonesianaMuhammad Hamzah AsadullahОценок пока нет
- The Effects of Menopause On The Serum Lipid Profile of Normal Females of South East Nigeria J. C. Igweh, I. U. Nwagha, J. M. OkaroДокумент6 страницThe Effects of Menopause On The Serum Lipid Profile of Normal Females of South East Nigeria J. C. Igweh, I. U. Nwagha, J. M. OkaroutarinuОценок пока нет
- How You Can Prevent and Reverse Heart Disease PDFДокумент3 страницыHow You Can Prevent and Reverse Heart Disease PDFAlmir Macario Barros50% (2)
- Hyperlipidemic Animal Models: Hyperlipidemia Induction Animal Specificity Modelsystem Effect RefДокумент2 страницыHyperlipidemic Animal Models: Hyperlipidemia Induction Animal Specificity Modelsystem Effect RefAwais Arain AhmadОценок пока нет
- Chapter 23 Drugs For HyperlipidemiaДокумент61 страницаChapter 23 Drugs For HyperlipidemiaIchsan FajriОценок пока нет
- SBAR ExampleДокумент1 страницаSBAR Examplekellymk2584100% (1)
- European Heart JournalДокумент50 страницEuropean Heart JournalAgustin CОценок пока нет
- Balance Review InfoДокумент17 страницBalance Review Infoapi-236004993100% (1)
- Exercise S10Документ25 страницExercise S10Mohamed MansourОценок пока нет
- Mineral and vitamin deficiency symptoms guideДокумент11 страницMineral and vitamin deficiency symptoms guidehaskellb572093% (15)
- Journal About OatДокумент8 страницJournal About OatHegar JoОценок пока нет
- Drug StudyДокумент4 страницыDrug StudySharwen_R_Rome_5572Оценок пока нет
- Coronary artery diseases reviewДокумент43 страницыCoronary artery diseases reviewKeputrian FKUPОценок пока нет
- Okra (Abelmoschus Esculentus L. Moench) As Anti-Cholesterol, Anti-Diabetic and Anti-Obesity in White Male RatsДокумент5 страницOkra (Abelmoschus Esculentus L. Moench) As Anti-Cholesterol, Anti-Diabetic and Anti-Obesity in White Male RatsSabrina JonesОценок пока нет
- Two-Day Meal Plan For Type II Diabetic and Cardiovascular PatientДокумент11 страницTwo-Day Meal Plan For Type II Diabetic and Cardiovascular Patientapi-301376054Оценок пока нет