Вам также может понравиться
- Case Study - Diabetes Mellitus (Nutrition&Dietetics)Документ10 страницCase Study - Diabetes Mellitus (Nutrition&Dietetics)Summer Suarez100% (1)
- Type 2 Diabetes MellitusДокумент19 страницType 2 Diabetes MellitusFelipe Senn Guerrero100% (2)
- Trading Floors WSДокумент86 страницTrading Floors WSAlok Singh100% (3)
- Dharnish ReportДокумент13 страницDharnish Reportdarshan75% (4)
- Referat Type 2 DMДокумент9 страницReferat Type 2 DMAyu Abharina PratiwiОценок пока нет
- Prediction of Type 2 Diabetes: A Natural History PerspectiveДокумент9 страницPrediction of Type 2 Diabetes: A Natural History Perspectiveandree_zz4890Оценок пока нет
- Pathogenesis of Type 2 Diabetes MellitusДокумент44 страницыPathogenesis of Type 2 Diabetes MellitusAsmat BurhanОценок пока нет
- Diabetes 1Документ22 страницыDiabetes 1aparna shamaОценок пока нет
- Case 2Документ23 страницыCase 2EJ CorpusОценок пока нет
- Pathogenesis of Type 2 Diabetes Mellitus - UpToDateДокумент26 страницPathogenesis of Type 2 Diabetes Mellitus - UpToDateMelina AranaОценок пока нет
- Type 2 Diabetes MellitusДокумент24 страницыType 2 Diabetes Mellitusdr. M.F. Romdhoni100% (1)
- Use of Acarbose Medan April 2010Документ14 страницUse of Acarbose Medan April 2010Ibnu WPОценок пока нет
- Molecular Basis of Type 2 DiabetesДокумент22 страницыMolecular Basis of Type 2 DiabetespimpellerОценок пока нет
- LEADING ARTICLE Insulin Resistance As A Predictor of Worsening of Glucose Tolerance in Type 2 DMДокумент6 страницLEADING ARTICLE Insulin Resistance As A Predictor of Worsening of Glucose Tolerance in Type 2 DMEvaPuspitaSariОценок пока нет
- Type 1 Diabetes Mellitus (Type 1 DM) : 1. Describe Patof Insulin PD DMДокумент5 страницType 1 Diabetes Mellitus (Type 1 DM) : 1. Describe Patof Insulin PD DMTheddyon BhenlieОценок пока нет
- Metabolic Changes in Diabetes: R. D. G. Leslie LondonДокумент4 страницыMetabolic Changes in Diabetes: R. D. G. Leslie LondonManuОценок пока нет
- Diabetes IIДокумент3 страницыDiabetes IIbangboomboomОценок пока нет
- Pathogenesis of Type 2 Diabetes Mellitus - UpToDateДокумент38 страницPathogenesis of Type 2 Diabetes Mellitus - UpToDatealinetibes1Оценок пока нет
- 1 Octeto de DefronzoДокумент23 страницы1 Octeto de DefronzoLesli Rodriguez50% (2)
- Pathogenesis and Pathophysiology of Diabetes MellitusДокумент4 страницыPathogenesis and Pathophysiology of Diabetes MellitusIka HabelОценок пока нет
- Review Article: Glucocorticoids and Type 2 Diabetes: From Physiology To PathologyДокумент10 страницReview Article: Glucocorticoids and Type 2 Diabetes: From Physiology To PathologyRengganis PutriОценок пока нет
- Clinical Review 102 Type 2 Diabetes Mellitus: Update On Diagnosis, Pathophysiology, and TreatmentДокумент7 страницClinical Review 102 Type 2 Diabetes Mellitus: Update On Diagnosis, Pathophysiology, and TreatmentWyn AgustinОценок пока нет
- Supplementary Information To Chapter 24: Review: Diabetes MellitusДокумент11 страницSupplementary Information To Chapter 24: Review: Diabetes MellitusAaron JoseОценок пока нет
- Costa Rica GlucoseДокумент91 страницаCosta Rica GlucoseAnthony HarderОценок пока нет
- Articulo Tacticas de Insulina en D2Документ30 страницArticulo Tacticas de Insulina en D2AlderkjОценок пока нет
- Diabetes Mellitus - Type 2 DiabetesДокумент11 страницDiabetes Mellitus - Type 2 DiabetesHafiz IbrahimОценок пока нет
- Livro Robbins PathologyДокумент18 страницLivro Robbins Pathologyernestooliveira50% (2)
- From The Triumvirate To The Ominous Octet: A New Paradigm For The Treatment of Type 2 Diabetes MellitusДокумент26 страницFrom The Triumvirate To The Ominous Octet: A New Paradigm For The Treatment of Type 2 Diabetes MellituselftotalОценок пока нет
- Trerapi Insulin Siip 2Документ10 страницTrerapi Insulin Siip 2Indra YudaОценок пока нет
- Diabetes Mellitus 1Документ16 страницDiabetes Mellitus 1Ajet AsaniОценок пока нет
- Glucose, Part1Документ33 страницыGlucose, Part1SarahОценок пока нет
- Resolving The Paradox of Hepatic Insulin ResistanceДокумент10 страницResolving The Paradox of Hepatic Insulin ResistanceMauro Rojas ZúñigaОценок пока нет
- Pancreatic Hormones and The Treatment of Diabetes MellitusДокумент46 страницPancreatic Hormones and The Treatment of Diabetes MellitusasmaОценок пока нет
- Etiopathogenesis of Type 2 DiabetesДокумент50 страницEtiopathogenesis of Type 2 Diabetesakash kondapalliОценок пока нет
- Pathology Assignment G 4Документ12 страницPathology Assignment G 4Hailat GОценок пока нет
- 二型糖尿病胰岛素分泌功能障碍 代谢异常的作用英文Документ12 страниц二型糖尿病胰岛素分泌功能障碍 代谢异常的作用英文慧吉Оценок пока нет
- Diabetes Diabetes Diabetes: ClassificationДокумент10 страницDiabetes Diabetes Diabetes: ClassificationAjay Pal NattОценок пока нет
- Insulin Resistance.:) DocxДокумент2 страницыInsulin Resistance.:) DocxHerbert Shirov Tendido SecurataОценок пока нет
- GI and Reproductive HormoneДокумент74 страницыGI and Reproductive Hormonepranutan739Оценок пока нет
- Targeting Postprandial HyperglycaemiaДокумент9 страницTargeting Postprandial HyperglycaemiaIbnu WPОценок пока нет
- Diabetes MellitusДокумент19 страницDiabetes MellitusHaleelu Abdul JaleelОценок пока нет
- Pharmacological Management of Type 2 Diabetes Mellitus: Rationale For Rational Use of InsulinДокумент9 страницPharmacological Management of Type 2 Diabetes Mellitus: Rationale For Rational Use of InsulinAditya Rachman Van Der ArjunaqueeОценок пока нет
- DM Report1Документ16 страницDM Report1Wendy EscalanteОценок пока нет
- Pathophysiology ScribdДокумент8 страницPathophysiology ScribdTamil VillardoОценок пока нет
- Hyperglycemia in Critical Illness: A ReviewДокумент11 страницHyperglycemia in Critical Illness: A ReviewSreejith ViswanathanОценок пока нет
- Ally Omary Mwambela MD2Документ10 страницAlly Omary Mwambela MD2Ally OmaryОценок пока нет
- Diagnosis Inggris PDFДокумент10 страницDiagnosis Inggris PDFMuhammad AbiyasaОценок пока нет
- Managemen Pasien Diabetes Mellitus Di Prosthodonsia: Agustin Wulan Suci DДокумент6 страницManagemen Pasien Diabetes Mellitus Di Prosthodonsia: Agustin Wulan Suci DYULYA DWI KARTIKASARIОценок пока нет
- Agustin Wulan PDFДокумент6 страницAgustin Wulan PDFCapaya AntrОценок пока нет
- Managemen Pasien Diabetes Mellitus Di Prosthodonsia: Agustin Wulan Suci DДокумент6 страницManagemen Pasien Diabetes Mellitus Di Prosthodonsia: Agustin Wulan Suci DYULYA DWI KARTIKASARIОценок пока нет
- Diabetes MellitusДокумент26 страницDiabetes Mellitusstrangefruit2483Оценок пока нет
- Dibetes FinalДокумент50 страницDibetes FinalPiyusha SharmaОценок пока нет
- Diabetes Millitus PDFДокумент41 страницаDiabetes Millitus PDFAbdullah BhattiОценок пока нет
- Comprehensive TreatmДокумент13 страницComprehensive TreatmRuki HartawanОценок пока нет
- Bab 2 OkДокумент28 страницBab 2 OknafitrawindriОценок пока нет
- Aims and ObjectivesДокумент13 страницAims and Objectivesmamun183Оценок пока нет
- Hypoglycemia and Hyperglycemia GM Eng 2022Документ3 страницыHypoglycemia and Hyperglycemia GM Eng 2022kabulkabulovich5Оценок пока нет
- Patho DMДокумент2 страницыPatho DMJohn Carlo SamsonОценок пока нет
- Nursing Care Plans For Diabetes MellitusДокумент12 страницNursing Care Plans For Diabetes MellitusPuteri AzmanОценок пока нет
- International Textbook of Diabetes MellitusОт EverandInternational Textbook of Diabetes MellitusR. A. DeFronzoОценок пока нет
- Consent For MTP PDFДокумент4 страницыConsent For MTP PDFMajid SheikhОценок пока нет
- Introduction of BiologyДокумент28 страницIntroduction of BiologyAlfin DestaОценок пока нет
- Restitution of Conjugal RightsДокумент3 страницыRestitution of Conjugal Rightsvalerian fernandesОценок пока нет
- N4 Fortran Codes For Computing The Space-Time Correlations of Turbulent Flow in A ChannelДокумент47 страницN4 Fortran Codes For Computing The Space-Time Correlations of Turbulent Flow in A Channelabhi71127112Оценок пока нет
- Trends in Computer-Based Second Language Assessment Jamieson 2005Документ15 страницTrends in Computer-Based Second Language Assessment Jamieson 2005Oana CarciuОценок пока нет
- M 1.2 RMДокумент16 страницM 1.2 RMk thejeshОценок пока нет
- Comparative and Superlative AdjectivesДокумент11 страницComparative and Superlative AdjectivesUri Leandro MuñozОценок пока нет
- Home DepotДокумент13 страницHome DepotTyfanie PetersenОценок пока нет
- Headache PAINДокумент1 страницаHeadache PAINOmarОценок пока нет
- The World of The GerДокумент302 страницыThe World of The GerMystic Master0% (1)
- Introduction To Qualitative ResearchДокумент19 страницIntroduction To Qualitative ResearchAnonymous LToOBqDОценок пока нет
- Picaresque Novel B. A. Part 1 EnglishДокумент3 страницыPicaresque Novel B. A. Part 1 EnglishIshan KashyapОценок пока нет
- Sonnet 39 ArticleДокумент2 страницыSonnet 39 ArticlelalyitaОценок пока нет
- Absolute Community of Property vs. Conjugal Partnership of GainsДокумент7 страницAbsolute Community of Property vs. Conjugal Partnership of GainsJill LeaОценок пока нет
- Discoid Lupus Erythematosus - Background, Etiology, EpidemiologyДокумент8 страницDiscoid Lupus Erythematosus - Background, Etiology, EpidemiologyJair MathewsОценок пока нет
- MKT202 Ga Su23Документ4 страницыMKT202 Ga Su23Như Nguyễn QuỳnhОценок пока нет
- CS302 - Lab Manual - Week No PDFДокумент8 страницCS302 - Lab Manual - Week No PDFattiqueОценок пока нет
- Film Viewing RomeroДокумент3 страницыFilm Viewing RomeroJenesis MuescoОценок пока нет
- Perceived Impact of Community Policing On Crime Prevention and Public Safety in Ozamiz CityДокумент7 страницPerceived Impact of Community Policing On Crime Prevention and Public Safety in Ozamiz Cityjabezgaming02Оценок пока нет
- IHL 1 BALLB ProjectДокумент16 страницIHL 1 BALLB Projectabcde fghikjОценок пока нет
- Reconceptualising Smart CitiesДокумент80 страницReconceptualising Smart CitiesDevang Parekh100% (1)
- Reading Exercise 2Документ2 страницыReading Exercise 2Park Hanna100% (1)
- E-Tech DLL Blank - Lesson 2-Nov 20-23Документ3 страницыE-Tech DLL Blank - Lesson 2-Nov 20-23Julie Ann SuarezОценок пока нет
- History of English Culture and Literature MidДокумент4 страницыHistory of English Culture and Literature Midfirdasalsa59Оценок пока нет
- FIDP Business Ethics and Social Responsibility PDFДокумент7 страницFIDP Business Ethics and Social Responsibility PDFRachell Mae Bondoc 1Оценок пока нет
- Subordinating Clause - Kelompok 7Документ6 страницSubordinating Clause - Kelompok 7Jon CamОценок пока нет
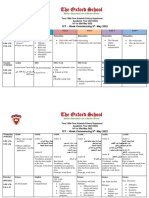
- Term 3 Mid-Term Assessment ScheduleДокумент9 страницTerm 3 Mid-Term Assessment ScheduleRabia MoeedОценок пока нет
- GR 148311-2005-In The Matter of The Adoption of StephanieДокумент8 страницGR 148311-2005-In The Matter of The Adoption of StephanieBogart CalderonОценок пока нет