Вам также может понравиться
- Aeymon Atlas of Common EYE DiseasesДокумент140 страницAeymon Atlas of Common EYE DiseasesAsma SikanderОценок пока нет
- ConstipationДокумент11 страницConstipationAsma SikanderОценок пока нет
- SleДокумент893 страницыSleAsma Sikander100% (4)
- 异位妊娠2011Документ65 страниц异位妊娠2011Asma SikanderОценок пока нет
- Kdigo-Gn-Guideline GN PDFДокумент143 страницыKdigo-Gn-Guideline GN PDFFerry JuniansyahОценок пока нет
- 09 前置胎盘Документ87 страниц09 前置胎盘Asma SikanderОценок пока нет
- Id & Cs Material LogДокумент4 страницыId & Cs Material LogAsma SikanderОценок пока нет
- Toxicology: General Aspects, Types, Routes of Exposure & AnalysisДокумент76 страницToxicology: General Aspects, Types, Routes of Exposure & AnalysisAsma SikanderОценок пока нет
- History of Trigonometry - Origins and DevelopmentДокумент10 страницHistory of Trigonometry - Origins and DevelopmentAsma SikanderОценок пока нет
- MRCP SyllabusДокумент145 страницMRCP SyllabusCalvinОценок пока нет
- Hypertensive Disorders of PregnancyДокумент59 страницHypertensive Disorders of PregnancyAsma SikanderОценок пока нет
- 1000 Prometric MCQ Solved 2Документ351 страница1000 Prometric MCQ Solved 2chronos653490% (105)
- FilzaДокумент1 страницаFilzaAsma SikanderОценок пока нет
- Short QДокумент53 страницыShort QAsma SikanderОценок пока нет
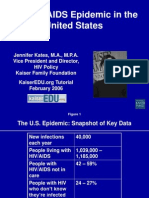
- The HIV/AIDS Epidemic in The United StatesДокумент27 страницThe HIV/AIDS Epidemic in The United StatesAsma SikanderОценок пока нет
- F The Normal and Abnormal Transformation ZoneДокумент6 страницF The Normal and Abnormal Transformation ZoneAsma SikanderОценок пока нет
- The HIV/AIDS Epidemic in The United StatesДокумент27 страницThe HIV/AIDS Epidemic in The United StatesAsma SikanderОценок пока нет
- It Has Been My Experience That Maximizing Income Is A Helluva Lot Less Important Than Maximizing Passion and Fulfillment in Your Both Professionally and PersonallyДокумент1 страницаIt Has Been My Experience That Maximizing Income Is A Helluva Lot Less Important Than Maximizing Passion and Fulfillment in Your Both Professionally and PersonallyAsma SikanderОценок пока нет
- Medical Record 2Документ7 страницMedical Record 2Asma SikanderОценок пока нет
- Viral Hepatitis: Yonghong Zhang M.D. D.Phil. Beijing Youan Hospital Capital Medical UniversityДокумент41 страницаViral Hepatitis: Yonghong Zhang M.D. D.Phil. Beijing Youan Hospital Capital Medical UniversityAsma SikanderОценок пока нет
- New Microsoft Office Word DocumentДокумент2 страницыNew Microsoft Office Word DocumentAsma SikanderОценок пока нет
- Viral Hepatitis: Yonghong Zhang M.D. D.Phil. Beijing Youan Hospital Capital Medical UniversityДокумент41 страницаViral Hepatitis: Yonghong Zhang M.D. D.Phil. Beijing Youan Hospital Capital Medical UniversityAsma SikanderОценок пока нет
- Chchinese 1Документ2 страницыChchinese 1Asma SikanderОценок пока нет
- Hemorrhagic Fever With Renal Syndrome: Duan Zhongping MDДокумент68 страницHemorrhagic Fever With Renal Syndrome: Duan Zhongping MDAsma SikanderОценок пока нет
- Ricardo A. Caicedo, MD: Pediatric Gastroenterology University of FloridaДокумент20 страницRicardo A. Caicedo, MD: Pediatric Gastroenterology University of FloridaAsma SikanderОценок пока нет
- 5 SyphilisДокумент35 страниц5 SyphilisAsma SikanderОценок пока нет
- Examination On Infectious Diseases For Capital Medical University 200X Batch Overseas StudentsДокумент2 страницыExamination On Infectious Diseases For Capital Medical University 200X Batch Overseas StudentsAsma SikanderОценок пока нет
- 2 Cranialz and Sensory Motor and CaseДокумент90 страниц2 Cranialz and Sensory Motor and CaseAsma SikanderОценок пока нет
- NeuroДокумент3 страницыNeuroAsma SikanderОценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- Manual Bilirubin TestДокумент2 страницыManual Bilirubin TestJorge Tapia MartínezОценок пока нет
- Pathology (Digestive System)Документ20 страницPathology (Digestive System)chepie villalonОценок пока нет
- Inborn Errors of Metabolism in Infancy: A Guide To DiagnosisДокумент11 страницInborn Errors of Metabolism in Infancy: A Guide To DiagnosisEdu Diaperlover São PauloОценок пока нет
- Problem Solving With AnswersДокумент50 страницProblem Solving With Answersapi-3814958Оценок пока нет
- Clinical Microscopy ReviewerДокумент31 страницаClinical Microscopy ReviewerbokbokbokОценок пока нет
- Correlation Between Neonatal Hyperbilirubinemia and Vitamin D Levels: A Meta-AnalysisДокумент12 страницCorrelation Between Neonatal Hyperbilirubinemia and Vitamin D Levels: A Meta-AnalysisAbdurrahman HasanuddinОценок пока нет
- Oral Medicine Journal Reading: Supervisor: Riani Setiadhi, DRG, SP - PM Presenter: Low Tee EngДокумент25 страницOral Medicine Journal Reading: Supervisor: Riani Setiadhi, DRG, SP - PM Presenter: Low Tee EngGabriel LowОценок пока нет
- Nursing Clinical Self-Directed LearningДокумент4 страницыNursing Clinical Self-Directed LearningDyan Bianca Suaso LastimosaОценок пока нет
- Diagnostic Report: PreliminaryДокумент7 страницDiagnostic Report: PreliminaryAyush Kumar GuptaОценок пока нет
- Liver Function Test InterpretationДокумент89 страницLiver Function Test InterpretationprashanthshamОценок пока нет
- Krok I 2013-17 ExplainedДокумент292 страницыKrok I 2013-17 ExplainedU1GoKu0% (1)
- 04 Liver Function Tests InterpretationДокумент45 страниц04 Liver Function Tests InterpretationDina HushamОценок пока нет
- ALTL enДокумент3 страницыALTL enyolanda0811Оценок пока нет
- PAEDIATRIC HANDBOOK GUIDE FOR COMMON ILLNESSESДокумент10 страницPAEDIATRIC HANDBOOK GUIDE FOR COMMON ILLNESSESAbdullah Al - JubairОценок пока нет
- Maternal Wellness Midterm ReviewДокумент144 страницыMaternal Wellness Midterm ReviewBethrice MelegritoОценок пока нет
- Baby Taber Case StudyДокумент13 страницBaby Taber Case StudytaylaОценок пока нет
- Pathophysiology - Obstructive JaundiceДокумент3 страницыPathophysiology - Obstructive JaundiceAbigail Lonogan0% (1)
- Pediatrics Summary 1996Документ126 страницPediatrics Summary 1996abdelaheem arabiatОценок пока нет
- Egyptian Neonatology Protocol 1st Ed 2022Документ124 страницыEgyptian Neonatology Protocol 1st Ed 2022sherif ghazyОценок пока нет
- Bile Production - Constituents - TeachMePhysiologyДокумент2 страницыBile Production - Constituents - TeachMePhysiologynotesom44Оценок пока нет
- Clinical Skills III: Gastrointestinal SystemДокумент39 страницClinical Skills III: Gastrointestinal Systemstella pangestikaОценок пока нет
- SANDRA, Apollo OBG Minor Disorders in Neonates PPT - SECTION BДокумент15 страницSANDRA, Apollo OBG Minor Disorders in Neonates PPT - SECTION Bsandra0% (1)
- NICU Cheat SheetДокумент4 страницыNICU Cheat SheetRichelle FrondaОценок пока нет
- Evaluation of abnormal liver function tests: a concise reviewДокумент6 страницEvaluation of abnormal liver function tests: a concise reviewMario Alberto RamosОценок пока нет
- Dermatologic Exam GuideДокумент3 страницыDermatologic Exam GuideJessica Febrina WuisanОценок пока нет
- Guideline HiperbilirubinemiaДокумент20 страницGuideline HiperbilirubinemiaCaroline LimaОценок пока нет
- POCTДокумент24 страницыPOCTHiminОценок пока нет
- Activity Xi - Serum and Plasma PrepartionДокумент3 страницыActivity Xi - Serum and Plasma PrepartionJorelle NogoyОценок пока нет
- Bosentan PI PDFДокумент12 страницBosentan PI PDFlaghatechinmayОценок пока нет
- Building materials guideДокумент31 страницаBuilding materials guideAhmad FitriОценок пока нет