Вам также может понравиться
- Cardiology EmergencyДокумент352 страницыCardiology EmergencyNoavilОценок пока нет
- Cardiac DisordersДокумент15 страницCardiac Disordersgold_enriquez100% (3)
- Valvular Heart DiseaseДокумент54 страницыValvular Heart DiseaseRommanah AzmiОценок пока нет
- Slide Pemeriksaan FisikДокумент26 страницSlide Pemeriksaan FisikAnindya AgrasidiОценок пока нет
- Cardiovascular ExaminationДокумент38 страницCardiovascular Examinationdrskdcrdio601250% (2)
- Ventricel Septal DefectДокумент38 страницVentricel Septal DefectzaipullahОценок пока нет
- Book Reading-Heart Disease Braunwald: Chapter 4 Physical Examination of The Heart and Circulation (I)Документ29 страницBook Reading-Heart Disease Braunwald: Chapter 4 Physical Examination of The Heart and Circulation (I)Jerrod WilsonОценок пока нет
- Assessment of Cardiovascular2014Документ12 страницAssessment of Cardiovascular2014alphabennydelta4468Оценок пока нет
- Left Ventricular FailureДокумент17 страницLeft Ventricular Failurenisha24100% (1)
- Valvular Heart DiseaseДокумент55 страницValvular Heart Diseaseapi-19916399Оценок пока нет
- Heart Murmurs: Kiran DhaliwalДокумент42 страницыHeart Murmurs: Kiran Dhaliwaltigermonkey100% (1)
- Approach To Patients With Possible Cardiovascular Disease and Physical Examination of The Cardiovascular SystemДокумент79 страницApproach To Patients With Possible Cardiovascular Disease and Physical Examination of The Cardiovascular SystemLajel S. LachicaОценок пока нет
- CHF FC III Ec Mitral StenosisДокумент36 страницCHF FC III Ec Mitral Stenosisbroken18bear100% (1)
- Cardiovascular ExaminationДокумент54 страницыCardiovascular ExaminationsankethОценок пока нет
- Cardiovascular ExaminationДокумент37 страницCardiovascular ExaminationmulatumeleseОценок пока нет
- New HematologyOncology FAE2016Документ108 страницNew HematologyOncology FAE2016omarОценок пока нет
- Ischemic Heart Diseases: Clinical Session: Prof. Ahmed Tamara, MD Dr. Mahmoud Baraka, MDДокумент28 страницIschemic Heart Diseases: Clinical Session: Prof. Ahmed Tamara, MD Dr. Mahmoud Baraka, MDNouran AliОценок пока нет
- 03 Cardiovascular System Examination FinalДокумент49 страниц03 Cardiovascular System Examination FinalYared TJОценок пока нет
- Mitral RegurgitationДокумент43 страницыMitral Regurgitationraissasafitry100% (1)
- Valvular Heart Disease: Joko AnggoroДокумент53 страницыValvular Heart Disease: Joko AnggoroReza SatriaОценок пока нет
- Rheumatic Valvular Heart Diseases by Prof DR N.K ChopraДокумент61 страницаRheumatic Valvular Heart Diseases by Prof DR N.K ChopraAbdulsalam DostОценок пока нет
- Cardiac ImagingДокумент27 страницCardiac ImagingViorelVelenciucОценок пока нет
- Heart FailureДокумент37 страницHeart FailureAmjad SobehОценок пока нет
- Congestive Heart Failure: Adopted From: Jarrod Eddy, PGY2 Internal Medicine Sub-I Lecture SeriesДокумент27 страницCongestive Heart Failure: Adopted From: Jarrod Eddy, PGY2 Internal Medicine Sub-I Lecture Serieskarika70Оценок пока нет
- Cardio-Vascular Disease: Mitral Stenosis & Mitral RegurgitationДокумент25 страницCardio-Vascular Disease: Mitral Stenosis & Mitral Regurgitationyulia silviОценок пока нет
- Cardio AssessmentДокумент104 страницыCardio Assessmentlowell.cerezo.ihsОценок пока нет
- Cardiovascular Assessment: Structure and FunctionДокумент16 страницCardiovascular Assessment: Structure and FunctionChin SilverОценок пока нет
- Examination and Investigation of The Cardiovascular System (CVS)Документ27 страницExamination and Investigation of The Cardiovascular System (CVS)Jake MillerОценок пока нет
- CVS Examination EditedДокумент134 страницыCVS Examination EditedThilak JayalathОценок пока нет
- 6. Митральные пороки. Клиника, диагностика, лечениеДокумент42 страницы6. Митральные пороки. Клиника, диагностика, лечениеabarna abiОценок пока нет
- 4 - Toronto Notes 2011 - Cardiology - and - Cardiovascular - SurgeryДокумент60 страниц4 - Toronto Notes 2011 - Cardiology - and - Cardiovascular - Surgeryqobsar100% (1)
- Cardiovascular History Taking and Physical ExaminationsДокумент35 страницCardiovascular History Taking and Physical ExaminationsEndalk AsfawОценок пока нет
- Health & Physical Assessment in Nursing: Cardiovascular SystemДокумент87 страницHealth & Physical Assessment in Nursing: Cardiovascular SystemNintu SomjiОценок пока нет
- Heart Failure: Definition, Etiology and PathophysiologyДокумент108 страницHeart Failure: Definition, Etiology and PathophysiologySianipar RomulussОценок пока нет
- Radiology of Cardiac and Vascular Structures: Cindy Chan, MDДокумент64 страницыRadiology of Cardiac and Vascular Structures: Cindy Chan, MDMohamoud MohamedОценок пока нет
- CVS Examination-1Документ84 страницыCVS Examination-1Prasenjit DasОценок пока нет
- Cardiovascular Pathology FINALДокумент45 страницCardiovascular Pathology FINALIanОценок пока нет
- Mitral Stenosis (MS) X Mitral Regurgitasi (MR)Документ25 страницMitral Stenosis (MS) X Mitral Regurgitasi (MR)Nur Faydotus SalsabilaОценок пока нет
- Cardiovascular SystemДокумент61 страницаCardiovascular SystemShimmering MoonОценок пока нет
- Congestive Heart Failure NYHA III and Non ST-elevation (Autosaved)Документ34 страницыCongestive Heart Failure NYHA III and Non ST-elevation (Autosaved)Laurencia ViolettaОценок пока нет
- Approach To Cardiovascular DiseaseДокумент23 страницыApproach To Cardiovascular DiseasesanjivdasОценок пока нет
- EmergencyДокумент47 страницEmergencymedstudy123Оценок пока нет
- Inspection and Palpation of The HeartДокумент38 страницInspection and Palpation of The Heartstudymedic100% (2)
- Valvular Heart DiseasesДокумент32 страницыValvular Heart DiseasesChrystel Mae PañaresОценок пока нет
- Physical Assessment of Cardiovascular SystemДокумент31 страницаPhysical Assessment of Cardiovascular SystemaagОценок пока нет
- Assessment Cardiac SystemДокумент51 страницаAssessment Cardiac Systemejarnmd100% (2)
- Heart DefectДокумент41 страницаHeart Defectdevutty 123Оценок пока нет
- Heart Failure: Vinawine P N 405100104Документ55 страницHeart Failure: Vinawine P N 405100104wennyОценок пока нет
- Heart Failure 1Документ50 страницHeart Failure 1dhiraj parmar100% (1)
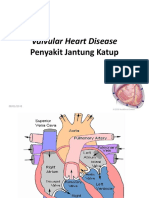
- Valvular Heart Disease: Penyakit Jantung KatupДокумент40 страницValvular Heart Disease: Penyakit Jantung KatupinhaОценок пока нет
- Cardiomegaly, RadiologyДокумент20 страницCardiomegaly, RadiologyJia LingОценок пока нет
- My-MRCP-notes-st1 and 3 by Dr-NadimДокумент93 страницыMy-MRCP-notes-st1 and 3 by Dr-NadimSaidunnessa IrinОценок пока нет
- Valvular Heart DiseaseДокумент42 страницыValvular Heart DiseaseareeparambilОценок пока нет
- Valvular Heart Disease. KulДокумент60 страницValvular Heart Disease. KulIntan Kumalasari RambeОценок пока нет
- Cardiovascular Examination SchemeДокумент5 страницCardiovascular Examination SchemeMuhammad Farhan KhaliqОценок пока нет
- #2 Cardiac AssessmentДокумент7 страниц#2 Cardiac AssessmentrunnermnОценок пока нет
- Tricuspid StenosisДокумент10 страницTricuspid StenosisRaiganОценок пока нет
- 5 - Cardio, RespiДокумент287 страниц5 - Cardio, RespiBeth CuntapayОценок пока нет
- Immediate Life Support for healthcare Practitioners: A Step-By-Step GuideОт EverandImmediate Life Support for healthcare Practitioners: A Step-By-Step GuideОценок пока нет
- Mu Trash MariДокумент22 страницыMu Trash MariVenkatesan VidhyaОценок пока нет
- MutraghatamДокумент26 страницMutraghatamVenkatesan Vidhya100% (3)
- Chap 40Документ5 страницChap 40Venkatesan VidhyaОценок пока нет
- 4.trigeminal Neuralgia OverviewДокумент5 страниц4.trigeminal Neuralgia OverviewVenkatesan VidhyaОценок пока нет
- KAZHUTHUVALIДокумент1 страницаKAZHUTHUVALIVenkatesan VidhyaОценок пока нет
- BronchitisДокумент3 страницыBronchitisVenkatesan VidhyaОценок пока нет
- Bells Palsy - PrincipleДокумент4 страницыBells Palsy - PrincipleVenkatesan VidhyaОценок пока нет
- Proverbs: Elderly The Doctor DoctorДокумент2 страницыProverbs: Elderly The Doctor DoctorVenkatesan VidhyaОценок пока нет
- Tests For Diabetic Nephropathy - StudiesДокумент2 страницыTests For Diabetic Nephropathy - StudiesVenkatesan VidhyaОценок пока нет
- 5.temporal Arteritis - More Med WTH Yogam KVДокумент4 страницы5.temporal Arteritis - More Med WTH Yogam KVVenkatesan VidhyaОценок пока нет
- VDVДокумент5 страницVDVVenkatesan VidhyaОценок пока нет
- When Are MRI Scans Used?: Brain Aneurysms Stroke Tumors of The BrainДокумент1 страницаWhen Are MRI Scans Used?: Brain Aneurysms Stroke Tumors of The BrainVenkatesan VidhyaОценок пока нет
- Rasayanam Dosage 47 Chapter - Chitraka Rasayanam Brain - QuotesДокумент1 страницаRasayanam Dosage 47 Chapter - Chitraka Rasayanam Brain - QuotesVenkatesan VidhyaОценок пока нет
- MutraghatamДокумент26 страницMutraghatamVenkatesan Vidhya100% (3)
- Bala Jeerakadi Is A Kashayam For Svasa KasaДокумент5 страницBala Jeerakadi Is A Kashayam For Svasa KasaVenkatesan VidhyaОценок пока нет
- SelvanДокумент144 страницыSelvanVenkatesan Vidhya100% (3)
- SKM ArticleДокумент17 страницSKM ArticleVenkatesan Vidhya75% (4)
- ManjuДокумент6 страницManjuVenkatesan VidhyaОценок пока нет
- What Is BrucellosisДокумент6 страницWhat Is BrucellosisVenkatesan VidhyaОценок пока нет
- Cluster 3 Radiographic Positioning and Radiologic Procedures Dec 2021 1Документ11 страницCluster 3 Radiographic Positioning and Radiologic Procedures Dec 2021 1Janelle Ann CasuyonОценок пока нет
- Brochure Finecare Plus Fs-114Документ2 страницыBrochure Finecare Plus Fs-114lumira Bogota100% (1)
- DNB Pediatrics - MCQ DNB Pediatics - December 2015Документ7 страницDNB Pediatrics - MCQ DNB Pediatics - December 2015Manju Manjunath100% (1)
- Cardiomyopathy Case StudyДокумент11 страницCardiomyopathy Case StudyJen Faye Orpilla100% (1)
- Complications Dialysis 12 09Документ47 страницComplications Dialysis 12 09irish_meg316557100% (2)
- Microbio Log BookДокумент14 страницMicrobio Log BookSahnusha SryenОценок пока нет
- برزنتيشن المدكلДокумент15 страницبرزنتيشن المدكلHuhgg VgctОценок пока нет
- Acute and Chronic InflammationДокумент52 страницыAcute and Chronic Inflammationjames20123100% (1)
- Acosta, Joyce Ara T. Week 7 & 8 Drug StudyДокумент11 страницAcosta, Joyce Ara T. Week 7 & 8 Drug StudyJoyce Ara Tumbaga AcostaОценок пока нет
- Health DeclarationДокумент8 страницHealth DeclarationmkwinijoanОценок пока нет
- TAMBALДокумент4 страницыTAMBALVianca Kate MarquezОценок пока нет
- Basic Elements of Medical Terms Word ElementsДокумент2 страницыBasic Elements of Medical Terms Word ElementsDANIELLE MAE F CASTROОценок пока нет
- Soap Notes HypertensionДокумент6 страницSoap Notes HypertensionCHRISTINE KARENDIОценок пока нет
- Vital SIgns - First Responder - August 2013 - v2.3Документ18 страницVital SIgns - First Responder - August 2013 - v2.3Rayan JaafeerОценок пока нет
- Covid - 19 Pre-Embarkation ChecklistДокумент2 страницыCovid - 19 Pre-Embarkation ChecklistSarah Grace BaltazarОценок пока нет
- Pdoc - DS Inflagic 20Документ3 страницыPdoc - DS Inflagic 20reshad reswaanОценок пока нет
- 2018 Krok2Документ10 страниц2018 Krok2mohamed esamОценок пока нет
- Nej Me 2300120Документ2 страницыNej Me 2300120choco cookiesОценок пока нет
- Cardiovascular Disease BrochureДокумент2 страницыCardiovascular Disease BrochureKawooya Ismael100% (1)
- Journal of Food Biochemistry - 2022 - Rana - Health Benefits of Polyphenols A Concise ReviewДокумент24 страницыJournal of Food Biochemistry - 2022 - Rana - Health Benefits of Polyphenols A Concise ReviewGustavoTorresОценок пока нет
- Chen2023Документ11 страницChen2023Mohamed MohammedОценок пока нет
- Heart DiseaseДокумент11 страницHeart Diseaseapi-529065933Оценок пока нет
- 342 - Hematology Physiology) Erythropoiesis Red Blood Cell FormationДокумент6 страниц342 - Hematology Physiology) Erythropoiesis Red Blood Cell Formationhasanatiya41Оценок пока нет
- داش دايت.fДокумент8 страницداش دايت.fesraaelkordy60Оценок пока нет
- Anatomy & Physiology of Cardiovascular & Respiratory SystemДокумент34 страницыAnatomy & Physiology of Cardiovascular & Respiratory SystemSalman KhanОценок пока нет
- Thoracic cavity & contents: Thorax Unit Lecture 3 & 4 مسعلأا ليلج رديح .دДокумент18 страницThoracic cavity & contents: Thorax Unit Lecture 3 & 4 مسعلأا ليلج رديح .دMuhammad UsmanОценок пока нет
- CardiologyДокумент62 страницыCardiologyLaura Kathrine Simpson92% (12)
- Congenital Heart Disease Made EasyДокумент30 страницCongenital Heart Disease Made EasyChristian HarnatОценок пока нет
- BNP, CRP, PCT in Sepstic BurnsДокумент7 страницBNP, CRP, PCT in Sepstic BurnsSagar MhetreОценок пока нет
- RCSI Handbook of Clinical Medicine - V1, 2nd EdДокумент574 страницыRCSI Handbook of Clinical Medicine - V1, 2nd EdRebecca Marshall86% (7)