Вам также может понравиться
- ICU Construction EssentialsДокумент91 страницаICU Construction EssentialsShimmering MoonОценок пока нет
- Leadership & MGTДокумент128 страницLeadership & MGTmutegeki nathanОценок пока нет
- FR Dur I Ski'ta - S: SK Ti 25-f $kifiДокумент6 страницFR Dur I Ski'ta - S: SK Ti 25-f $kifijerayne50% (2)
- Missing Persons Policy SummaryДокумент16 страницMissing Persons Policy SummaryAgnieszka WaligóraОценок пока нет
- Ed Assessment Tool SampleДокумент28 страницEd Assessment Tool SampleAnonymous ibmeej9Оценок пока нет
- Healthcare Environmental Services A Complete Guide - 2020 EditionОт EverandHealthcare Environmental Services A Complete Guide - 2020 EditionОценок пока нет
- Administrative Policy for Hospital AdmissionsДокумент8 страницAdministrative Policy for Hospital AdmissionsHAMMYER ALROKHAMIОценок пока нет
- TRIAGE POLICIES JuvyДокумент6 страницTRIAGE POLICIES JuvyCuyapo Infirmary Lying-In HospitalОценок пока нет
- Emergency CodesДокумент23 страницыEmergency CodesJennifer B. GarciaОценок пока нет
- Hospitalist Program Toolkit: A Comprehensive Guide to Implementation of Successful Hospitalist ProgramsОт EverandHospitalist Program Toolkit: A Comprehensive Guide to Implementation of Successful Hospitalist ProgramsОценок пока нет
- Toledo Code Blue PolicyДокумент4 страницыToledo Code Blue PolicySt SОценок пока нет
- Nursing Services Manual AIIMSДокумент91 страницаNursing Services Manual AIIMSpraveenjenaОценок пока нет
- 001 Admission APP MED 001Документ7 страниц001 Admission APP MED 001HAMMYER ALROKHAMIОценок пока нет
- Cardio & PulmoДокумент64 страницыCardio & PulmoAnonymous bgB7IhОценок пока нет
- Surgical Site Marking PolicyДокумент11 страницSurgical Site Marking PolicymiraОценок пока нет
- Blood Transfusions - TGH Policies & ProceduresДокумент4 страницыBlood Transfusions - TGH Policies & ProceduresMark Anthony FranciscoОценок пока нет
- JD Ward Clerk Job DescriptionДокумент2 страницыJD Ward Clerk Job DescriptionMD Luthfy LubisОценок пока нет
- Nursing Skill RevisionДокумент1 страницаNursing Skill RevisionMichelle TseОценок пока нет
- PACU Discharge CriteriaДокумент1 страницаPACU Discharge CriteriaTarquin Tomada100% (2)
- Scripps Hospital Patient Visitor Policy PDFДокумент2 страницыScripps Hospital Patient Visitor Policy PDFcode4saleОценок пока нет
- Nss 505 Medical Surgical Nursing Critical Care I Teacher - Co .KeДокумент171 страницаNss 505 Medical Surgical Nursing Critical Care I Teacher - Co .Kebirhanu Ayenew AnleyОценок пока нет
- Duties and Responsibilities of An RN: Lpns CnasДокумент4 страницыDuties and Responsibilities of An RN: Lpns CnasSPTDОценок пока нет
- IV Complications Signs, Prevention, TreatmentДокумент6 страницIV Complications Signs, Prevention, TreatmentMercicae AОценок пока нет
- Procedure Manual HospitalДокумент196 страницProcedure Manual HospitalMarian StrihaОценок пока нет
- Liabilities of HospitalsДокумент36 страницLiabilities of HospitalsMJ Carreon100% (1)
- Recovery Room NurseДокумент5 страницRecovery Room NurseChristin 'Kirei' AndoloОценок пока нет
- How To Move The Patient From The Bed To The Wheelchair How To Move The Patient From The Bed To The WheelchairДокумент9 страницHow To Move The Patient From The Bed To The Wheelchair How To Move The Patient From The Bed To The WheelchairAfniy ApriliaОценок пока нет
- Patient Safety Organization A Complete Guide - 2020 EditionОт EverandPatient Safety Organization A Complete Guide - 2020 EditionОценок пока нет
- Clinical Services Plan TTM SamoaДокумент69 страницClinical Services Plan TTM SamoajohnkornieОценок пока нет
- A&E Triage SystemДокумент5 страницA&E Triage SystemArnel AlmutiahОценок пока нет
- 2 Critical Care UnitДокумент59 страниц2 Critical Care UnitPALMA , JULIA A.Оценок пока нет
- Out Patient DepartmentДокумент5 страницOut Patient DepartmentShikhaОценок пока нет
- Western Australian Patient Identification Policy PDFДокумент14 страницWestern Australian Patient Identification Policy PDFpuspadiniaОценок пока нет
- CLCGP030 Theatre Operating List Session Scheduling PolicyДокумент19 страницCLCGP030 Theatre Operating List Session Scheduling PolicyJeffy PuruggananОценок пока нет
- Emergency Drugs (LEAD)Документ8 страницEmergency Drugs (LEAD)RayePrudenteОценок пока нет
- The COAT & Review Approach: How to recognise and manage unwell patientsОт EverandThe COAT & Review Approach: How to recognise and manage unwell patientsРейтинг: 5 из 5 звезд5/5 (1)
- IV Cannulation ChecklistДокумент2 страницыIV Cannulation ChecklistDo0odi AlharbiОценок пока нет
- Arero Primary Hospital Triage Protocol Nov 2022Документ4 страницыArero Primary Hospital Triage Protocol Nov 2022sami ketemaОценок пока нет
- TransitionДокумент13 страницTransitionDonna NituraОценок пока нет
- ISBAR Communication ToolДокумент16 страницISBAR Communication ToolTni JolieОценок пока нет
- Nurse Bob's MICU/CCU Survival Guide Critical Care Concepts General Nursing Requirements of The Intensive Care PatientДокумент7 страницNurse Bob's MICU/CCU Survival Guide Critical Care Concepts General Nursing Requirements of The Intensive Care Patientlil' princessОценок пока нет
- Critical Transport GuidelinesДокумент22 страницыCritical Transport GuidelinesFadil RamadhanОценок пока нет
- DR, OR, WardДокумент14 страницDR, OR, WardjanОценок пока нет
- Manual For EndosДокумент19 страницManual For EndosVarsha MalikОценок пока нет
- Oral Care in ICUДокумент8 страницOral Care in ICUYani Va-Rhy100% (1)
- Delivery InstrumentsДокумент1 страницаDelivery InstrumentsKristine Dianne San BuenaventuraОценок пока нет
- Acute Nutrition PolicyДокумент79 страницAcute Nutrition PolicyyohaneskoОценок пока нет
- Equipments in Icu: Mr. Amol Temkar Asso. Prof College of NursingДокумент46 страницEquipments in Icu: Mr. Amol Temkar Asso. Prof College of NursingAmol TemkarОценок пока нет
- Today Admissions Discharge FON Sem-1 2021Документ25 страницToday Admissions Discharge FON Sem-1 2021zakiralihussaini786Оценок пока нет
- Guide to Measuring Vital SignsДокумент32 страницыGuide to Measuring Vital SignsJacqueline de AsisОценок пока нет
- prehospital-EMS-COVID-19-recommendations - 4.4Документ19 страницprehospital-EMS-COVID-19-recommendations - 4.4MEONEОценок пока нет
- KPI Discussion Paper 3Документ22 страницыKPI Discussion Paper 3Manager HR Hijaz Hospital100% (1)
- Police Hospital PolicyДокумент3 страницыPolice Hospital PolicyThe Salt Lake TribuneОценок пока нет
- Clinical Guidelines For Management of HTNДокумент6 страницClinical Guidelines For Management of HTNChaturangaNSenerath100% (1)
- Transfer Using Gait Belt PDFДокумент2 страницыTransfer Using Gait Belt PDFJasonJejametОценок пока нет
- 1 - 10 - 209case Report-Methanol Intoxication Complicated With Acute Pancreatitis Alcoholic Ketoacidosis and Intracranial HemorrhageДокумент3 страницы1 - 10 - 209case Report-Methanol Intoxication Complicated With Acute Pancreatitis Alcoholic Ketoacidosis and Intracranial HemorrhageEdah HumaidahОценок пока нет
- Prevalens 2014 FranceДокумент9 страницPrevalens 2014 FranceEdah HumaidahОценок пока нет
- Immune Thrombocitopeni PurpuraДокумент8 страницImmune Thrombocitopeni PurpuraEdah HumaidahОценок пока нет
- Lynne Graham Damiano S Return by Lynne Graham PDFДокумент90 страницLynne Graham Damiano S Return by Lynne Graham PDFEdah Humaidah88% (16)
- Angela Aki TegamiДокумент5 страницAngela Aki TegamiEdah HumaidahОценок пока нет
- Jurnal Karies Gigi Pada AnakДокумент11 страницJurnal Karies Gigi Pada AnakYock HeadShooter0% (1)
- SympathiДокумент2 страницыSympathiEdah HumaidahОценок пока нет
- Laporan Kasus Kegawatdaruratan Intoksikasi Metanol: Oleh: Edah HumaidahДокумент1 страницаLaporan Kasus Kegawatdaruratan Intoksikasi Metanol: Oleh: Edah HumaidahEdah HumaidahОценок пока нет
- Angela Aki TegamiДокумент5 страницAngela Aki TegamiEdah HumaidahОценок пока нет
- 2011 ITP Pocket GuideДокумент8 страниц2011 ITP Pocket GuidevtОценок пока нет
- International Headache Classification III ICHD III 2013 Beta 1Документ180 страницInternational Headache Classification III ICHD III 2013 Beta 1Fityan Aulia RahmanОценок пока нет
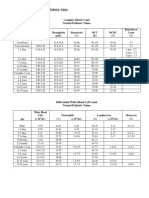
- 30a2131 Complete Blood Count Normal Pediatric Values PDFДокумент1 страница30a2131 Complete Blood Count Normal Pediatric Values PDFReziel Basilan Manalo100% (2)
- Vascular Trauma and Its ManagementДокумент5 страницVascular Trauma and Its ManagementEdah HumaidahОценок пока нет
- International Headache Classification III ICHD III 2013 Beta 1Документ180 страницInternational Headache Classification III ICHD III 2013 Beta 1Fityan Aulia RahmanОценок пока нет
- F.3 Ocd 072012Документ17 страницF.3 Ocd 072012Edah Humaidah100% (1)
- Epidemiology and Outcome of Vascular Trauma at A British Major Trauma CentreДокумент7 страницEpidemiology and Outcome of Vascular Trauma at A British Major Trauma CentreEdah HumaidahОценок пока нет
- Whatyouneed 09 1Документ24 страницыWhatyouneed 09 1Edah HumaidahОценок пока нет
- Existing Trauma and Critical Care Scoring SystemsДокумент8 страницExisting Trauma and Critical Care Scoring SystemsEdah HumaidahОценок пока нет
- Anesthesia For LaparosДокумент12 страницAnesthesia For LaparosEdah HumaidahОценок пока нет
- Hellp Syndr, SibaiДокумент21 страницаHellp Syndr, SibaiMohamed MukhrizОценок пока нет
- WhenДокумент3 страницыWhenEdah HumaidahОценок пока нет
- Penelitian LepraДокумент13 страницPenelitian LepraEdah HumaidahОценок пока нет
- Acute Diare WHO 2005Документ50 страницAcute Diare WHO 2005Boby Abdul RahmanОценок пока нет
- Steroid LepraДокумент20 страницSteroid LepraEdah HumaidahОценок пока нет
- Acute Diare WHO 2005Документ50 страницAcute Diare WHO 2005Boby Abdul RahmanОценок пока нет
- Institutional Biosafety Committee: Role of TheДокумент14 страницInstitutional Biosafety Committee: Role of TheSyeda Wardah NoorОценок пока нет
- Metabolic Stress PDFДокумент30 страницMetabolic Stress PDFNurul Latifa MuhammadОценок пока нет
- Henrietta Lacks: Dr. Roz Iasillo Trinity High School River Forest, ILДокумент13 страницHenrietta Lacks: Dr. Roz Iasillo Trinity High School River Forest, ILRoz IasilloОценок пока нет
- Chapter 17 Reproductive SystemДокумент15 страницChapter 17 Reproductive SystemJurugo GodfreyОценок пока нет
- Knee Osteoarthritis A Review of LiteratureДокумент8 страницKnee Osteoarthritis A Review of LiteratureKurnia Elka VidyarniОценок пока нет
- Examination of Bacterial Contamination in Blood ComponentsДокумент21 страницаExamination of Bacterial Contamination in Blood ComponentsCik KahadiОценок пока нет
- Pre-Eclampsia and EclampsiaДокумент21 страницаPre-Eclampsia and EclampsiaTamratKelelegn100% (1)
- Smoking and Hypertension - UpToDateДокумент25 страницSmoking and Hypertension - UpToDatemehdi.chlif4374Оценок пока нет
- A Glossary of Anesthetic Jargon .8Документ4 страницыA Glossary of Anesthetic Jargon .8TonyОценок пока нет
- Case Pre 2Документ11 страницCase Pre 2Juviely PremacioОценок пока нет
- Tinnitus Today December 1998 Vol 23, No 4Документ29 страницTinnitus Today December 1998 Vol 23, No 4American Tinnitus AssociationОценок пока нет
- Mudlark CPI Medical Care Report Oct 09Документ8 страницMudlark CPI Medical Care Report Oct 09MudlarkResearchОценок пока нет
- Parenteral Nutrition CalculationsДокумент62 страницыParenteral Nutrition CalculationsaqeelaadnanОценок пока нет
- Evmlu Uganda.2020Документ124 страницыEvmlu Uganda.2020ALINOMUGASHA EMMANUELОценок пока нет
- Postnatal Care at The Health Post and in The CommunityДокумент23 страницыPostnatal Care at The Health Post and in The CommunityGreggy Francisco LaraОценок пока нет
- Standard Surgical Attire Surgical ScrubДокумент20 страницStandard Surgical Attire Surgical ScrubzekkipianoОценок пока нет
- MENSTRUAL HYGIENE KNOWLEDGE AMONG STUDENTSДокумент11 страницMENSTRUAL HYGIENE KNOWLEDGE AMONG STUDENTSElsa Christy GumayОценок пока нет
- Empagliflozin Metformin HCL: Jardiance Duo®Документ2 страницыEmpagliflozin Metformin HCL: Jardiance Duo®Lord Carlo CabangalОценок пока нет
- HIV Drug ChartДокумент5 страницHIV Drug Chartalejandroo_26Оценок пока нет
- Nursing Fundamentals Exam ReviewДокумент10 страницNursing Fundamentals Exam ReviewAlain CheryОценок пока нет
- Anaesthetic Considerations for Day Care SurgeryДокумент8 страницAnaesthetic Considerations for Day Care SurgerySirisha Ckv100% (1)
- Comorbidities of Hearing Loss and The Implications of Multimorbidity For Audiological Care. Hearing Research - 10.1016:j.heares.2018.06.008Документ12 страницComorbidities of Hearing Loss and The Implications of Multimorbidity For Audiological Care. Hearing Research - 10.1016:j.heares.2018.06.008ALEIRAMGONZALEZОценок пока нет
- MrdicДокумент18 страницMrdicpapa0011Оценок пока нет
- EphedraДокумент9 страницEphedraapi-367367047Оценок пока нет
- Olimpiada Engleza 2017 CL A 8A PDFДокумент4 страницыOlimpiada Engleza 2017 CL A 8A PDFAnthony AdamsОценок пока нет
- Introduction to Pakistan's National Essential Drug ListДокумент16 страницIntroduction to Pakistan's National Essential Drug ListUmair MazharОценок пока нет
- Discharge PlanДокумент4 страницыDischarge PlanPaul Loujin LeeОценок пока нет
- Kanker Payudara: Dr. Dian Andriani, SPKK, M.Biomed, MarsДокумент31 страницаKanker Payudara: Dr. Dian Andriani, SPKK, M.Biomed, Marsdian andriani ratna dewiОценок пока нет
- Legal and Ethical Issues in Psychiatric NursingДокумент38 страницLegal and Ethical Issues in Psychiatric NursingElizabeth McKee100% (2)
- Data Peserta Gartheting LT 3aumst Final 2022Документ11 страницData Peserta Gartheting LT 3aumst Final 2022Doni IrawanОценок пока нет