Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- 2016 MD Bond-$200k To Damascus HS Boosters For ArtTurfДокумент5 страниц2016 MD Bond-$200k To Damascus HS Boosters For ArtTurfConcussion_MCPS_MdОценок пока нет
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- NFL 2010 Letter Re Concussion LegДокумент2 страницыNFL 2010 Letter Re Concussion LegConcussion_MCPS_MdОценок пока нет
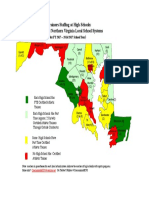
- Projected Athletic Trainer Staffing in FY 2017-Md, NoVA, and DCДокумент1 страницаProjected Athletic Trainer Staffing in FY 2017-Md, NoVA, and DCConcussion_MCPS_MdОценок пока нет
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- MCPS Sports Concussion Data 2014-15Документ1 страницаMCPS Sports Concussion Data 2014-15Concussion_MCPS_MdОценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Parent Letter To MCPS Re Student Injury Data - 01-14-2015Документ11 страницParent Letter To MCPS Re Student Injury Data - 01-14-2015Concussion_MCPS_MdОценок пока нет
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- LCPS Response To Parents Re Inova-Brain Sentry Research ProposalДокумент2 страницыLCPS Response To Parents Re Inova-Brain Sentry Research ProposalConcussion_MCPS_MdОценок пока нет
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- MCPS Sports Concussion Data 2013-14Документ1 страницаMCPS Sports Concussion Data 2013-14Concussion_MCPS_MdОценок пока нет
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- MCPS Ath Trainer Staffing-FY2016 OpBdgt Summary P 40 of 73Документ73 страницыMCPS Ath Trainer Staffing-FY2016 OpBdgt Summary P 40 of 73Concussion_MCPS_MdОценок пока нет
- MCPS Staff Response To MoCo BOE Durso Q Re Concussion Jan-Feb 2014Документ2 страницыMCPS Staff Response To MoCo BOE Durso Q Re Concussion Jan-Feb 2014Concussion_MCPS_MdОценок пока нет
- MCPS Chart Showing Sports Concussions by Sport and by High School 2013-2014Документ1 страницаMCPS Chart Showing Sports Concussions by Sport and by High School 2013-2014Concussion_MCPS_MdОценок пока нет
- MCPS Response-Data Re Concussion and Other Injuries in High School Athletics 2013-2014Документ2 страницыMCPS Response-Data Re Concussion and Other Injuries in High School Athletics 2013-2014Concussion_MCPS_MdОценок пока нет
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Brain Sentry Inova Football Helmet Sensor Research Study ProposalДокумент5 страницBrain Sentry Inova Football Helmet Sensor Research Study ProposalConcussion_MCPS_MdОценок пока нет
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- MCPS (MD) Penalties For Tobacco Use at SchoolДокумент2 страницыMCPS (MD) Penalties For Tobacco Use at SchoolConcussion_MCPS_MdОценок пока нет
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- MCPS Systemwide Safety PRGM - Employee Injury Report 01-16-2014Документ9 страницMCPS Systemwide Safety PRGM - Employee Injury Report 01-16-2014Concussion_MCPS_MdОценок пока нет
- MPSSAA HeadsUp Media Release, 5-5-2014Документ1 страницаMPSSAA HeadsUp Media Release, 5-5-2014Concussion_MCPS_MdОценок пока нет
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Template 3-B, MCPS Athletics Injury Report-11 High School (From Athletic Trainer Data)Документ1 страницаTemplate 3-B, MCPS Athletics Injury Report-11 High School (From Athletic Trainer Data)Concussion_MCPS_MdОценок пока нет
- MCPS (MD) Parent Request For Sports Injuries Data 06-03-2014Документ6 страницMCPS (MD) Parent Request For Sports Injuries Data 06-03-2014Concussion_MCPS_MdОценок пока нет
- MCPS (MD) Tobacco-Free SCH PolicyДокумент2 страницыMCPS (MD) Tobacco-Free SCH PolicyConcussion_MCPS_MdОценок пока нет
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Minutes of MD ST BD of Ed Meeting, 4-22-2014Документ47 страницMinutes of MD ST BD of Ed Meeting, 4-22-2014Concussion_MCPS_MdОценок пока нет
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- PPE Ath W/ Special Needs-Suppl History FormДокумент1 страницаPPE Ath W/ Special Needs-Suppl History FormConcussion_MCPS_MdОценок пока нет
- Template 1-C, MCPS 25 High Schools Athletics Injury Report, 2013-2014Документ2 страницыTemplate 1-C, MCPS 25 High Schools Athletics Injury Report, 2013-2014Concussion_MCPS_MdОценок пока нет
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Template 3-A, MCPS Athletics Injury Report Each High School (From Athletic Trainer Data)Документ1 страницаTemplate 3-A, MCPS Athletics Injury Report Each High School (From Athletic Trainer Data)Concussion_MCPS_MdОценок пока нет
- Template 2-B, MCPS 25 High Schools Athletics Concussion Database Report, July 2013 - June 2014Документ1 страницаTemplate 2-B, MCPS 25 High Schools Athletics Concussion Database Report, July 2013 - June 2014Concussion_MCPS_MdОценок пока нет
- Template 1-B, MCPS Athletics Injury Reports 2013-2014Документ2 страницыTemplate 1-B, MCPS Athletics Injury Reports 2013-2014Concussion_MCPS_MdОценок пока нет
- MCPS Reg For Reporting Student InjuriesДокумент2 страницыMCPS Reg For Reporting Student InjuriesConcussion_MCPS_MdОценок пока нет
- Template 2-A, MCPS XXX High School Athletics Concussion Database Report, July 2013 - June 2014Документ1 страницаTemplate 2-A, MCPS XXX High School Athletics Concussion Database Report, July 2013 - June 2014Concussion_MCPS_MdОценок пока нет
- MCPS Systemwide Safety PRGM - Employee Injury Report 01-16-2014Документ9 страницMCPS Systemwide Safety PRGM - Employee Injury Report 01-16-2014Concussion_MCPS_MdОценок пока нет
- Template 1-A, MCPS Student Accident Report Injuries 7-1-2013-PresentДокумент1 страницаTemplate 1-A, MCPS Student Accident Report Injuries 7-1-2013-PresentConcussion_MCPS_MdОценок пока нет
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- MCPS Student Injury Report FormДокумент2 страницыMCPS Student Injury Report FormConcussion_MCPS_MdОценок пока нет
- HoCo MD BOE Agenda 01-23-14Документ2 страницыHoCo MD BOE Agenda 01-23-14Concussion_MCPS_MdОценок пока нет
- IICPДокумент38 страницIICPIntira Aom ChainapaengОценок пока нет
- Dari DausДокумент4 страницыDari DausSalmah YusufОценок пока нет
- Lit. Review MatrixДокумент10 страницLit. Review MatrixBobbyNicholsОценок пока нет
- Applications On Neurological and Neuropsychiatric Diseases: MembersДокумент14 страницApplications On Neurological and Neuropsychiatric Diseases: MembersNiobe LilithОценок пока нет
- BDRSДокумент4 страницыBDRSSiegfried CristoforОценок пока нет
- Chapter 10Документ19 страницChapter 10Natura ManilaОценок пока нет
- Nola Pender - Wikipedia PDFДокумент11 страницNola Pender - Wikipedia PDFAvhie ConcepcionОценок пока нет
- Environmental Enrichment and Neuronal Plasticity - Oxford HandbooksДокумент42 страницыEnvironmental Enrichment and Neuronal Plasticity - Oxford HandbooksAdela Fontana Di TreviОценок пока нет
- Cancer Pain ManagementДокумент22 страницыCancer Pain ManagementWanie Kaflee100% (1)
- Mental Toughness - The Only Way Out Is Through - 2ndskies ForexДокумент17 страницMental Toughness - The Only Way Out Is Through - 2ndskies ForexTheophilus GbadegesinОценок пока нет
- LIDZ THEODORE - A Psicosocial Orientation To Schizophrenic DisordersДокумент9 страницLIDZ THEODORE - A Psicosocial Orientation To Schizophrenic DisordersRodrigo G.Оценок пока нет
- Reasearch SummariesДокумент12 страницReasearch Summariesapi-508554918Оценок пока нет
- Cad Midterm BДокумент2 страницыCad Midterm BKhrisAngelPeñamanteОценок пока нет
- The Pomodoro TechniqueДокумент14 страницThe Pomodoro TechniquesmartguidesОценок пока нет
- Consumer Behaviour Implications For Marketing Strategy 7th Edition Quester Test BankДокумент31 страницаConsumer Behaviour Implications For Marketing Strategy 7th Edition Quester Test Bankselinajacob7nhlfu100% (29)
- Q&A OsloДокумент9 страницQ&A OslosyukriОценок пока нет
- KUSSNER MVI 24 Questions 2019 PDFДокумент11 страницKUSSNER MVI 24 Questions 2019 PDFChristian JaiderОценок пока нет
- Item Analysis and ValidationДокумент11 страницItem Analysis and Validationᜄᜓᜄᜓᜇᜀᜈᜄ ᜎᜒᜐᜓᜄᜀОценок пока нет
- Sandler, CountertransferenceandRole Responsiveness (34181)Документ12 страницSandler, CountertransferenceandRole Responsiveness (34181)María José Lamas100% (1)
- Speech AudiometryДокумент17 страницSpeech AudiometryPero Kvržica100% (1)
- Practice Test - Error IdentificationДокумент5 страницPractice Test - Error IdentificationTùng Lâm TrầnОценок пока нет
- KULIAH 1 - Introduction - 24september2012Документ37 страницKULIAH 1 - Introduction - 24september2012UNOОценок пока нет
- Dge Cience: Beyond NeuroscienceДокумент20 страницDge Cience: Beyond NeuroscienceCambiador de MundoОценок пока нет
- Verbal BehaviorДокумент38 страницVerbal BehaviorfelipemagalhaeslemosОценок пока нет
- Lesson 1 Nervous SystemДокумент3 страницыLesson 1 Nervous SystemDwayneGeraldОценок пока нет
- Promoting Work Life Balance Among Higher Learning Institution Employees: Does Emotional Intelligence Matter?Документ8 страницPromoting Work Life Balance Among Higher Learning Institution Employees: Does Emotional Intelligence Matter?Global Research and Development ServicesОценок пока нет
- Reflection of Psychology 1010Документ2 страницыReflection of Psychology 1010api-270635734Оценок пока нет
- Chapter 11-Sociocultural Theory & Contextual PerspectivesДокумент5 страницChapter 11-Sociocultural Theory & Contextual PerspectivesEmmanuel YuОценок пока нет
- The Nature of Oral CommunicationДокумент40 страницThe Nature of Oral CommunicationKate Evangelista100% (2)
- Facilitating Meaningful Learning ExperiencesДокумент3 страницыFacilitating Meaningful Learning ExperiencesNur SholihahОценок пока нет
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDОт EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDРейтинг: 5 из 5 звезд5/5 (1)
- Summary of The 4-Hour Body: An Uncommon Guide to Rapid Fat-Loss, Incredible Sex, and Becoming Superhuman by Timothy FerrissОт EverandSummary of The 4-Hour Body: An Uncommon Guide to Rapid Fat-Loss, Incredible Sex, and Becoming Superhuman by Timothy FerrissРейтинг: 4.5 из 5 звезд4.5/5 (81)
- The Bridesmaid: The addictive psychological thriller that everyone is talking aboutОт EverandThe Bridesmaid: The addictive psychological thriller that everyone is talking aboutРейтинг: 4 из 5 звезд4/5 (131)
- The Obesity Code: Unlocking the Secrets of Weight LossОт EverandThe Obesity Code: Unlocking the Secrets of Weight LossРейтинг: 4 из 5 звезд4/5 (6)
- Briefly Perfectly Human: Making an Authentic Life by Getting Real About the EndОт EverandBriefly Perfectly Human: Making an Authentic Life by Getting Real About the EndОценок пока нет