Вам также может понравиться
- Troubled Bodies: Critical Perspectives on Postmodernism, Medical Ethics, and the BodyОт EverandTroubled Bodies: Critical Perspectives on Postmodernism, Medical Ethics, and the BodyОценок пока нет
- Trusting Doctors: The Decline of Moral Authority in American MedicineОт EverandTrusting Doctors: The Decline of Moral Authority in American MedicineРейтинг: 4 из 5 звезд4/5 (2)
- The Changing Face of Medical Sociology: David WainwrightДокумент18 страницThe Changing Face of Medical Sociology: David WainwrightHelly Chane LeeОценок пока нет
- The End of MedicineДокумент5 страницThe End of Medicinejcamacho95Оценок пока нет
- Alternative Therapies: A Social and Ethical OverviewДокумент10 страницAlternative Therapies: A Social and Ethical OverviewjfjjfjfjjfjfОценок пока нет
- Sir Robert Hutchisons PetitionДокумент3 страницыSir Robert Hutchisons PetitionJeffrey ElvinОценок пока нет
- Understanding and Applying Medical Anthr (Pages 333-335) (2023!12!13)Документ4 страницыUnderstanding and Applying Medical Anthr (Pages 333-335) (2023!12!13)Rachel SawhОценок пока нет
- Beyond Medicalisation - N. RoseДокумент3 страницыBeyond Medicalisation - N. RoseManuel Guerrero Antequera100% (1)
- Chapter 1 - Philosophy of Integrative Medicine - 2018 - Integrative MedicineДокумент11 страницChapter 1 - Philosophy of Integrative Medicine - 2018 - Integrative MedicineandreОценок пока нет
- De GruyterДокумент17 страницDe Gruyterisabella granataОценок пока нет
- Drug EducationДокумент12 страницDrug EducationKyle Santos100% (1)
- Quackonomics!: The Cost of Unscientific Health Care in the U.S. ...and Other Fraud Found Along the WayОт EverandQuackonomics!: The Cost of Unscientific Health Care in the U.S. ...and Other Fraud Found Along the WayОценок пока нет
- Our Present Complaint: American Medicine, Then and NowОт EverandOur Present Complaint: American Medicine, Then and NowРейтинг: 4.5 из 5 звезд4.5/5 (3)
- The Shape of Things To Come: Homage To H.G. Wells: Special ArticleДокумент5 страницThe Shape of Things To Come: Homage To H.G. Wells: Special ArticleTequila ChanОценок пока нет
- Obstacles To Medical Progress: S. S. SatchwellДокумент41 страницаObstacles To Medical Progress: S. S. SatchwellSexy888Оценок пока нет
- Tutorial - ETHICS - 01-01-P1&2 - Introduction To Ethics and Biomedical Ethics & Ethical Issues in Doctor-Patient RelationshipsДокумент43 страницыTutorial - ETHICS - 01-01-P1&2 - Introduction To Ethics and Biomedical Ethics & Ethical Issues in Doctor-Patient RelationshipsRenОценок пока нет
- Edgar Cayce's SecretДокумент9 страницEdgar Cayce's Secretpwdtx007100% (1)
- INTRO MEDICAL BIOETHICSДокумент16 страницINTRO MEDICAL BIOETHICSorsibogi100% (1)
- Rethinking Medical Ethics: A View From Below: Paul Farmer and Nicole Gastineau CamposДокумент25 страницRethinking Medical Ethics: A View From Below: Paul Farmer and Nicole Gastineau CamposMaria Teresa CaneteОценок пока нет
- Rationalism and Empiricism in Modern MedicineДокумент18 страницRationalism and Empiricism in Modern MedicineAzhily Jones HisolerОценок пока нет
- Medical Myths and Quack Practices in a Cavite CommunityДокумент11 страницMedical Myths and Quack Practices in a Cavite CommunityShennymae Pelayo100% (3)
- Doctor Does Not Know Best: Why in The New Century Physicians Must Stop Trying To Benefit PatientsДокумент22 страницыDoctor Does Not Know Best: Why in The New Century Physicians Must Stop Trying To Benefit PatientsColesniuc AdinaОценок пока нет
- Radical Health_AbstractsДокумент16 страницRadical Health_AbstractsFabianeVinenteОценок пока нет
- Jonas, Waine B. - Manual de Terapias AlternativasДокумент348 страницJonas, Waine B. - Manual de Terapias AlternativaspauloadrianoОценок пока нет
- 30.08.22 - All Medicine Is SocialДокумент4 страницы30.08.22 - All Medicine Is SocialPola PhotographyОценок пока нет
- Complementary and Alternative MedicineДокумент10 страницComplementary and Alternative MedicineSuneel Kotte100% (1)
- Cahill,-Lisa-sowle.2003.Bioethics Theology and Social ChangeДокумент36 страницCahill,-Lisa-sowle.2003.Bioethics Theology and Social ChangeisamarartОценок пока нет
- The Complementary Nature oДокумент5 страницThe Complementary Nature opsramОценок пока нет
- Commodification of Health CareДокумент5 страницCommodification of Health Caremadequal2658Оценок пока нет
- Medical ethics principles and branchesДокумент6 страницMedical ethics principles and branchesdobuol gorОценок пока нет
- Research Paper Medical AnthropologyДокумент7 страницResearch Paper Medical Anthropologymwjhkmrif100% (1)
- Medical Ethics GuideДокумент30 страницMedical Ethics GuideMohitraheja007Оценок пока нет
- Project Muse 18635Документ19 страницProject Muse 18635RODRIGUEZ BAÑOS JEYVERОценок пока нет
- Essential Issues in Complementary and Alternative Medicine: Definitional ConsiderationsДокумент34 страницыEssential Issues in Complementary and Alternative Medicine: Definitional ConsiderationsHayo HihiОценок пока нет
- Foucault and The Medicalisation Critique: Deborah LuptonДокумент17 страницFoucault and The Medicalisation Critique: Deborah LuptonLorena MariñoОценок пока нет
- NATURAL HEALING: A HOLISTIC APPROACHДокумент137 страницNATURAL HEALING: A HOLISTIC APPROACHAnjani KumarОценок пока нет
- TCM Dec 19 IssueДокумент15 страницTCM Dec 19 IssuepranajiОценок пока нет
- Asian Medical SystemsДокумент12 страницAsian Medical SystemsReggie ThorpeОценок пока нет
- De GruyterДокумент17 страницDe Gruytervince34Оценок пока нет
- Culture Illness and CareДокумент9 страницCulture Illness and CareIncaOreОценок пока нет
- Irving Zola - Article Review by Syed Ali Moiz PDFДокумент8 страницIrving Zola - Article Review by Syed Ali Moiz PDFali moizОценок пока нет
- Explanatory Model KleinmanДокумент10 страницExplanatory Model KleinmanartsiyantiОценок пока нет
- Medical Anthropology NoteДокумент37 страницMedical Anthropology NoteKeyeron DugumaОценок пока нет
- Health EssayДокумент15 страницHealth Essayanita violeta50% (2)
- DoctorsДокумент2 страницыDoctorsKing CaboiscoolОценок пока нет
- CM1 EXTRA 1978 Culture Illness and CareДокумент8 страницCM1 EXTRA 1978 Culture Illness and Careiancooke09Оценок пока нет
- Clinical Lessons From Anthropologic and Cross-Cultural ResearchДокумент11 страницClinical Lessons From Anthropologic and Cross-Cultural ResearchmohdrusydiОценок пока нет
- Complementary and Alternative MedicineДокумент7 страницComplementary and Alternative MedicinenaveenkhanalОценок пока нет
- George Vithoulkas' Insights on the Science of HomeopathyДокумент7 страницGeorge Vithoulkas' Insights on the Science of HomeopathyKurai Isabel PgОценок пока нет
- mhst1 1704Документ8 страницmhst1 1704AlexОценок пока нет
- Life without Disease: The Pursuit of Medical UtopiaОт EverandLife without Disease: The Pursuit of Medical UtopiaОценок пока нет
- Medicine, Anthropology, Community...Документ6 страницMedicine, Anthropology, Community...Gretel PeltoОценок пока нет
- NSG 106Документ12 страницNSG 106Anipah AmintaoОценок пока нет
- B Ing 4Документ19 страницB Ing 4Rivan 21Оценок пока нет
- Medical Nemesis: The Expropriation of Health (1976Документ19 страницMedical Nemesis: The Expropriation of Health (1976IamJmlingconОценок пока нет
- S1 Hippocratic Oath Seminar and Reading NotesДокумент7 страницS1 Hippocratic Oath Seminar and Reading NotesTaraSubba1995Оценок пока нет
- Roberto González Echevarría-Myth and Archive - A Theory of Latin American Narrative (Cambridge Studies in Latin American and Iberian Literature) (1990) PDFДокумент259 страницRoberto González Echevarría-Myth and Archive - A Theory of Latin American Narrative (Cambridge Studies in Latin American and Iberian Literature) (1990) PDFCristian TablazonОценок пока нет
- On MaterialДокумент4 страницыOn MaterialCristian TablazonОценок пока нет
- The Arrival - Shaun TanДокумент119 страницThe Arrival - Shaun TanCristian Tablazon91% (34)
- Historiography in the PhilippinesДокумент26 страницHistoriography in the PhilippinesJose Lester Correa Duria100% (1)
- Voice As A Technology of Selfhood: Towards An Analysis of Racialized Timbre and Vocal PerformanceДокумент305 страницVoice As A Technology of Selfhood: Towards An Analysis of Racialized Timbre and Vocal PerformanceCristian TablazonОценок пока нет
- Guiliana - Bruno Despre HAPTIC PDFДокумент14 страницGuiliana - Bruno Despre HAPTIC PDFBogdan Tanase-Marinescu100% (1)
- The Politics of EnvyДокумент22 страницыThe Politics of EnvyCristian TablazonОценок пока нет
- Aesthetics of Decay Sample ChapterДокумент10 страницAesthetics of Decay Sample ChapterryanmaloneОценок пока нет
- Jean Baudrillard, CollectingДокумент19 страницJean Baudrillard, CollectingLarisa OanceaОценок пока нет
- Freudian FetishДокумент13 страницFreudian FetishCristian TablazonОценок пока нет
- Biagioli Probing Limits RepresentationДокумент16 страницBiagioli Probing Limits RepresentationCristian TablazonОценок пока нет
- The Ecstacy of Communication - BaudrillardДокумент5 страницThe Ecstacy of Communication - BaudrillardMardawud JamiОценок пока нет
- Jean Baudrillard, CollectingДокумент19 страницJean Baudrillard, CollectingLarisa OanceaОценок пока нет
- Primates in ParadiseДокумент0 страницPrimates in ParadiseCristian TablazonОценок пока нет
- Week City MemoryДокумент57 страницWeek City MemoryCristian TablazonОценок пока нет
- Final 14 DreamsДокумент55 страницFinal 14 DreamsImpossible MikeОценок пока нет
- Five Poems: They Were WarnedДокумент5 страницFive Poems: They Were WarnedCristian TablazonОценок пока нет
- BilingДокумент6 страницBilingCristian TablazonОценок пока нет
- BlackholeДокумент15 страницBlackholeCristian Tablazon100% (2)
- Guide Questions For All ExperimentsДокумент7 страницGuide Questions For All ExperimentsRomar Angelo AvilaОценок пока нет
- A 32 Morosanu - Bioetica Si Tehnologie PDFДокумент3 страницыA 32 Morosanu - Bioetica Si Tehnologie PDFSergiu DobanОценок пока нет
- A Speech About AbortionДокумент1 страницаA Speech About AbortionYusei FudoОценок пока нет
- Fur Farm Intelligence Project: Full Article From Bite Back MagazineДокумент14 страницFur Farm Intelligence Project: Full Article From Bite Back Magazinefur_industry_docsОценок пока нет
- BrochureДокумент7 страницBrochureapi-596896646Оценок пока нет
- Schizophrenia Fact SheetДокумент1 страницаSchizophrenia Fact SheetAan KhaerismanОценок пока нет
- Mtlbe Lecture IntroductionДокумент11 страницMtlbe Lecture IntroductionAndrea Galang CruzОценок пока нет
- Medical Technology (MT) Laws: A. Basic ConceptsДокумент19 страницMedical Technology (MT) Laws: A. Basic ConceptsK-idol LiveОценок пока нет
- Nursing Technology: La Union Colleges of Science and Technology, IncДокумент2 страницыNursing Technology: La Union Colleges of Science and Technology, IncManny Daniel AbuanОценок пока нет
- Does Human Genome Editing Reinforce or Violate Human DignityДокумент8 страницDoes Human Genome Editing Reinforce or Violate Human DignityBadtz MaruОценок пока нет
- Bertino2022 Book ClinicalEthicsForConsultationPДокумент181 страницаBertino2022 Book ClinicalEthicsForConsultationPJonatán Pérez RochaОценок пока нет
- Research Paper On Mandatory VaccinesДокумент7 страницResearch Paper On Mandatory Vaccinesapi-569130786Оценок пока нет
- Impacts of GMOs on Philippine AgricultureДокумент3 страницыImpacts of GMOs on Philippine AgricultureIrish Cheska EspinosaОценок пока нет
- Bautista Resty. Module in GECETHДокумент77 страницBautista Resty. Module in GECETHDj22 JakeОценок пока нет
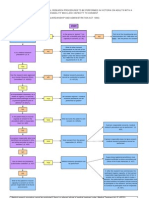
- Approval Process For Medical Research FlowchartДокумент1 страницаApproval Process For Medical Research FlowchartabcdcattigerОценок пока нет
- Previous BON Files (Leadership, Management, Bioethics and Research)Документ11 страницPrevious BON Files (Leadership, Management, Bioethics and Research)Tom CuencaОценок пока нет
- Project On Mercy KillingДокумент26 страницProject On Mercy KillingPranjal SrivastavaОценок пока нет
- Notes BIOETHICSДокумент3 страницыNotes BIOETHICSKim BadillesОценок пока нет
- Informative Speech Outlinerd Copy 2Документ7 страницInformative Speech Outlinerd Copy 2Aidil AzizОценок пока нет
- NCM 106 - HEALTH CARE ETHICS PRINCIPLESДокумент35 страницNCM 106 - HEALTH CARE ETHICS PRINCIPLESCorpus, Irene Zen P.100% (2)
- Ethical PrinciplesДокумент14 страницEthical PrinciplesRaees Shahid BasharatОценок пока нет
- Nur 104 Bioethics RbeДокумент36 страницNur 104 Bioethics RbeAelise Bacalso100% (1)
- REGISTERED GROOMING FACILITIES IN THE PHILIPPINESДокумент9 страницREGISTERED GROOMING FACILITIES IN THE PHILIPPINESEiflaRamosStaRitaОценок пока нет
- MJ1902 Ethics Brochure Paginated V4Документ12 страницMJ1902 Ethics Brochure Paginated V4yos_peace86Оценок пока нет
- 01 PRIVACY, CONFIDENTIALITY - EQUALITY TranscriptionДокумент3 страницы01 PRIVACY, CONFIDENTIALITY - EQUALITY TranscriptionCHRISTIAN ASHLEY PASCUAОценок пока нет
- (Advancing Global Bioethics 4) Henk a.M.J. Ten Have (Eds.) - Bioethics Education in A Global Perspective - Challenges in Global Bioethics (2015, Springer Netherlands)Документ221 страница(Advancing Global Bioethics 4) Henk a.M.J. Ten Have (Eds.) - Bioethics Education in A Global Perspective - Challenges in Global Bioethics (2015, Springer Netherlands)Marco Ivan AlmeidaОценок пока нет
- NCM 108 - Aug. 21, 2018Документ10 страницNCM 108 - Aug. 21, 2018rimeoznekОценок пока нет
- Ethics Handbook For Residents PDFДокумент254 страницыEthics Handbook For Residents PDFAloah122346Оценок пока нет
- Legal and Ethical Aspects of Organ Donation After Euthanasia in Belgium and The NetherlandsДокумент5 страницLegal and Ethical Aspects of Organ Donation After Euthanasia in Belgium and The NetherlandsThePoliticalHatОценок пока нет
- Fisher & Anushko, Research EthicsДокумент17 страницFisher & Anushko, Research Ethicsstar lightОценок пока нет
- Bioethics Activity - Aceres PDFДокумент4 страницыBioethics Activity - Aceres PDFS. C.Оценок пока нет