Академический Документы
Профессиональный Документы
Культура Документы
Protective cellular immunity against hepatitis C virus
Загружено:
Chelsey WilsonИсходное описание:
Оригинальное название
Авторское право
Доступные форматы
Поделиться этим документом
Поделиться или встроить документ
Этот документ был вам полезен?
Это неприемлемый материал?
Пожаловаться на этот документАвторское право:
Доступные форматы
Protective cellular immunity against hepatitis C virus
Загружено:
Chelsey WilsonАвторское право:
Доступные форматы
Immunology and Cell Biology (2006) 84, 239249
doi:10.1111/j.1440-1711.2006.01427.x
Review Article
Protective immunity against hepatitis C virus infection
L I S A N E L L I O T T,1,2 A N D R E W R L L OY D ,2 J O H N B Z I E G L E R 1 a n d R O S E M A RY A F F R E N C H 1,3
1
School of Womens and Childrens Health and 2Inflammatory Diseases Research Unit, School of Medical Sciences, The University of New South Wales, Sydney, New South Wales and 3Viral Immunology Group, Burnet Institute, Melbourne, Victoria, Australia
Summary There is increasing evidence that a small percentage of individuals exposed to the hepatitis C virus have the capacity to generate a strong cellular immune response against the virus and avoid persistent infection, and perhaps do so repeatedly after re-exposure. This article reviews the evidence that the responses identified in this unique group of individuals represent the protective immunity that will need to be elicited by hepatitis C virus vaccines. Key words: cellular immunity, hepatitis C virus, vaccination.
Introduction
Although protection from infection is the primary goal of preventive vaccination, in reality, protective vaccines generally seek to dramatically minimize the number of cells that become infected, rather than to absolutely prevent infection of any host cell. Most vaccines for prevention of viral infections induce strong antibody responses to neutralize viral particles before target cells can become infected, or allow rapid control of viral replication to minimize subsequent cell to cell transmission.17 These mechanisms are most effective when significant concentrations of high-affinity antibodies are generated.8,9 The use of vaccines that seek solely to elicit an antibody response currently appears inadequate to either prevent or control at least two of the major human viral pandemics, namely infections due to HIV and hepatitis C virus (HCV). Both of these viruses circulate as a complex quasispecies and are able to rapidly mutate to evade immunological control. There are currently a number of HIV and HCV vaccine candidates that seek to elicit cellular immunity, including both CD4 helper and CD8 CTL responses directed against multiple viral Ag. These candidates cannot absolutely prevent infection given that viral replication in cellular targets must be established before viral Ag can be presented to CTL, either through classical MHC class I restricted pathways or through cross-presentation. Accordingly, the goal of these vaccines is to prevent the establishment of persistent infection. The great majority of primary infections with HCV are asymptomatic.10,11 However, unlike other flaviviruses related to HCV, and unlike hepatitis B virus (HBV), HCV causes chronic infection in 5080% of adults who are exposed to it, resulting in progressive fibrotic liver injury that may ultimately lead to cirrhosis, liver failure and an increased risk of hepatocellular carcinoma.1216 Following primary infection,
viral persistence occurs in most cases despite the generation of HCV-specific antibodies and cellular immune responses, indicating that the immune response is functionally ineffective in the majority of exposed individuals. Studies in humans, and in chimpanzees, which provide the sole animal model for HCV disease, have shown that even after successful viral clearance, the immune system is often unable to prevent reinfection with either homologous or heterologous strains of HCV.1721 Therefore, in the case of HCV protective immunity may be defined as the ability of the immune system to prevent the establishment of chronic infection after exposure to HCV, whether that protection be with the first encounter or with re-exposure after previous infection episodes. Against this backdrop, recent data from studies in both humans and chimpanzees have challenged the dogma of a largely ineffective immune response and suggested that a small subset of individuals exposed to HCV, perhaps repeatedly, may develop cellular immunity against the virus, which confers protection against persistent infection. These findings may be analogous to those obtained in the context of HIV suggesting protection in unique subgroups such as the exposed, but uninfected, Kenyan sex workers.22,23 Understanding the characteristics of this immune response may provide key insights relevant to HCV vaccine development.
The primary immune response to HCV
Although the determinants of successful clearance of primary infection should not necessarily be taken as indicative of protective immunity, or of the best pathway to vaccine development, understanding the characteristics of such responses is an appropriate first step. As most episodes of primary HCV infection in humans are asymptomatic and therefore largely unavailable for intensive immunological and virological studies, important data have been obtained from studies in chimpanzees. Although this model has provided critical insights into HCV pathogenesis, an important caveat in extrapolating data to human infection is that there is a higher rate of clearance in chimpanzees.24 In addition, the limited availability and high cost of chimpanzees leads to
Correspondence: Rosemary A Ffrench, Viral Immunology Group, Burnet Institute, Commercial Road, Prahran, Vic. 3004, Australia. Email: ffrench@burnet.edu.au Received 28 September 2005; accepted 22 December 2005. 2006 The Authors Journal compilation 2006 Australasian Society for Immunology Inc.
240
LN Elliott et al.
the publication of many studies that include sample sizes of only one or two chimpanzees.25,26
Humoral immune response
HCV-specific antibodies generally develop 28 weeks after exposure in humans and remain throughout the course of chronic infection. Antibody levels are generally low, with limited affinity maturation or isotype switching.27 In those who clear the virus, antibody levels gradually diminish in titre, with approximately 50% of individuals having no detectable antibodies by 20 years after primary infection.28,29 Although this humoral immunity may be part of an effective immune response in the minority of individuals who clear the primary infection, antibody generation is not an absolute requirement for viral clearance.3032 Studies have shown that individuals with hypogammaglobulinaemia clear the virus in proportions similar to the general population,3335 and recovery does not correlate to anti-HCV antibody titres or to the levels of antibodies directed to the envelope glycoproteins, E1 and E2,24,36,37 although it should be noted that these studies did not assess neutralizing antibodies. Both strain-specific and cross-reactive neutralizing antibodies against HCV have been identified in humans and chimpanzees.31,3842 High-titre neutralizing antibodies were able to protect chimpanzees from infection with homologous strains of HCV, but were ineffective against heterologous variants.31,40 The majority of chronically infected individuals develop cross-reactive neutralizing antibodies late in the course of primary infection, and this delay may be one of the mechanisms by which persistence occurs.38,41 Neutralizing antibodies were found in only two of seven acutely infected patients in a series of cases with primary infection, and their presence did not correlate to viral clearance,38 although the presence of neutralizing antibodies was associated with a decrease in viraemia.42 However, the presence of neutralizing antibodies in a commercial immune globulin preparation was associated with protection from HCV transmission, as infection only occurred in individuals using products that had been screened for HCV antibodies, suggesting that the exclusion had removed neutralizing antibodies.39 It is plausible that antibody development plays a role in the clearance of established viral variants, but fails to keep pace with emergent viral quasipecies.43 Persistence of an antibody response to HCV in chronic infection, like maintenance of strong CD8 responses, also depends on the presence of ongoing infection.44 It should be noted that assays used to detect neutralizing antibodies are based on pseudotyped virus and may only be able to reliably detect antibodies specific for that strain.
HCV genome have been able to detect responses in 60% of individuals with chronic infection.49 Responses in individuals with chronic infection are more narrowly directed and of a lower magnitude than those found in individuals who are able to clear the virus.49 Both CD4147,5052 and CD815359 responses appear to be required to control HCV infection. A strong, multispecific and sustained CD41 response has been associated with viral clearance,5052 with control of viraemia being inversely related to viral load.47 An increase in CD81 numbers has been associated with HCV-RNA levels5759 and effective immune control.5356 Chronic infection is associated with reduced or ineffective proliferation, antiviral cytokine production and lytic activity of CD41 and CD81 T cells.60,61 Viral clearance has been weakly associated with the class II MHC alleles DRB1 and DQB1 in a number of small ethnically restricted cohorts, suggesting that a superior ability to bind and present particular epitopes to CD41 cells may be important.6265 However, analysis of the specificity of CD81 CTL responses in 20 individuals who had cleared HCV showed that the dominant epitopes were highly varied, even among those sharing HLA alleles.49 This suggests that diverse responses directed against multiple epitopes are required to resolve primary infection. Consistent with this notion are data indicating that the emergence of CTL epitope variants early in the course of primary infection appears to contribute to HCV persistence.66
Protective immunity against HCV Reinfection
Early studies in the chimpanzee model showed that repeated exposure to heterologous and homologous strains of HCV can result in repeated episodes of acute hepatitis following each exposure, although reinfection was generally associated with reduced periods of viraemia.18,21 No difference between the humoral immune responses to heterologous and homologous challenges was identified, although cellular immune responses were not evaluated. It was concluded that natural infection does not prevent reinfection, producing early doubts about the feasibility of designing an effective HCV vaccine.18 More recent studies have shown that chimpanzees who had previously cleared HCV and were rechallenged did show an improved course of disease when compared with naive animals with primary infection. The re-exposed animals had reduced peak alanine aminotransferase levels, shorter periods of viraemia, lower peak HCV-RNA levels, as well as earlier production and higher levels of the antiviral cytokines IFN-g and TNF-a.19,20 In one study, rechallenged animals were viraemic for an average of 5 weeks, in comparison to the average of 14 weeks associated with primary infection.19 Rechallenged animals also had viral titres that were, on average, two logs lower than those recorded in the primary infection. HCVspecific cellular immune responses were detected in all animals within 2 weeks of rechallenge. Another study noted that rechallenged animals cleared the virus more rapidly despite the lack of antibodies to HCV envelope glycoproteins.20 Viral clearance rates following rechallenge in these animals have been correlated to the magnitude of the cellular immune responses generated after re-exposure. Animals with the most vigorous and sustained CD41 responses cleared viral RNA
Cellular immune response
Avigorous and broad cellular immune response early in primary infection has been associated with an increased likelihood of viral clearance,28,45,46 with responses found in 79100% of individuals who clear HCV, but in only 044% of those with chronic infection.29,47,48 However, these early assay systems predominantly used Ag based on the core and nonstructural (NS) viral protein NS3 sequences and were unable to detect responses directed against other HCV regions. In contrast, recent assays using overlapping peptides covering the entire
2006 The Authors. Journal compilation 2006 Australasian Society for Immunology Inc.
Immunity against hepatitis C virus
241
rapidly, whereas animals with weak CD41 responses had persistent, low levels of circulating RNA.67 Depletion studies have shown that both CD41 and CD81 T cells are essential in preventing chronic infection after rechallenge.58,68 These findings indicate that this relative protection after re-exposure in the chimpanzee model is primarily mediated by a cellular immune response, although these studies did not assess neutralizing antibodies. Recent data in humans also suggest that individuals who have previously cleared HCV infection are less likely to develop chronic infection after re-exposure.32 A cohort of 164 injecting drug users (IDU) who had not previously been infected with HCV (i.e. who were anti-HCV antibody negative) and 98 IDU who had previously cleared HCV (i.e. who were anti-HCV positive and HCV-RNA negative) were followed for a 2 year period. New episodes of viraemia were detected in 21% of the IDU without prior infection and in 12% of IDU who had cleared an earlier HCV infection. Individuals with primary infection were 12 times more likely to develop chronic infection, and had average HCV-RNA levels two logs higher than those who became infected after having previously cleared HCV. It should be noted, however, that these findings were not confirmed in the recent analysis of reinfection episodes in a retrospective cohort study of Australian IDU.69 Nevertheless, these data suggest that the immune system is sometimes able to generate responses that are at least partially protective against establishment of chronic infection. As detailed analysis of the humoral and cellular immune responses against HCV was not undertaken in either of these studies, the characteristics of the immune responses in the setting of reinfection warrant further study. In particular, the patterns of response in those who efficiently clear the viral infection, and in those who do not, remain unclear.
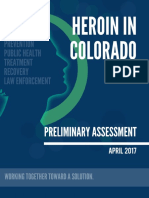
infection.7479 As documented prior exposure has not always been evident in the subjects in these studies, such individuals may be referred to as being seronegative immune (Fig. 1). CD41 lymphocytes from 4 of 20 (20%) healthy, uninfected spouses of chronically infected individuals were shown to proliferate in response to recombinant HCV proteins, particularly NS3.74 The responses were maintained on repeated testing and all individuals remained antibody and RNA negative over 1 year of follow up, indicating that none were in the early stages of HCV infection. HCV-specific CD41 and CD81
Acute infection with clearance
9 10 11 12
Time (months)
Persistent infection
Exposure to HCV without apparent infection
Development of CD81 CTL responses against viral Ag is generally taken to indicate that established infection has previously occurred with processing and presentation of viral peptides through class I MHC. Accordingly, the identification of anti-HCV-specific CTL responses in the blood or liver of individuals who do not have evidence of current infection (i.e. anti-HCV antibodies, abnormal liver function tests or detectable HCV-RNA) implies that these individuals are likely to have been previously infected with HCV. The antibody-negative status may result either from seroreversion or from an initial failure to develop an antibody response in association with the primary infection. With regard to the former, long-term follow up of recipients of HCV-contaminated blood products has shown that of those who clear the primary infection, approximately 50% serorevert to become HCV antibody negative when tested by ELISA over the following decade.28,70 The serological responses to individual HCV Ag detected by immunoblot generally diminish gradually, with an indeterminate profile becoming evident over time, followed by ultimate disappearance of all serological reactivity. In a minority of cases, a failure of antibody synthesis may result from a coexisting immunodeficiency state, such as HIV infection.7173 Several cross-sectional studies of groups of seronegative individuals who are at risk of exposure to HCV have identified evidence of cellular immunity against the virus in the absence of
9 10 11 12
Time (months)
High-risk seronegative immune
Re-exposure
Time (months)
9 10 11 12
Figure 1 Three possible outcomes of hepatitis C virus (HCV) exposure. (A) Acute or self-limiting infection is associated with a strong cellular immune response, the development of HCV-specific antibodies (Ab) and viral clearance. (B) Some individuals have an ineffective cellular immune response and despite periods of viral control, they are ultimately unable to clear the virus and develop chronic disease. (C) A small percentage of individuals are exposed to the virus and develop an effective cellular immune response, resulting in viral clearance with transient viraemia and without antibody production. Periods of viraemia are shaded. Episodes of re-exposure to the virus are indicated by arrows in panel C. d, RNA; n, T-cell response; j, Ab.
2006 The Authors. Journal compilation 2006 Australasian Society for Immunology Inc.
242
LN Elliott et al.
cellular immune responses were also identified in 2 of 10 laboratory personnel working in settings at risk for occupational exposure to HCV.75 It is possible that the peptide-induced CTL responses reported in these two subjects may have resulted from in vitro priming, as two rounds of prior stimulation with tetanus toxoid and IL-2 were used. However, the same two subjects (and none of the remaining eight individuals) also showed proliferative responses to several recombinant HCV proteins covering both structural and nonstructural regions. In another study, 7 of 29 (24%) seronegative individuals living with a chronically infected family member were found to have CTL responses directed against multiple HCV epitopes in a peptide-based [51Cr]-release assay using highly purified CD81 T cells.76 Limiting dilution analysis indicated that these precursor CTL were present in the circulation at very low or undetectable frequencies. However, HCV-specific effector CD81 T cells directed against both structural and nonstructural epitopes were found in four subjects (14%) from the same group when assessed by a sensitive enzyme-linked immunospot assay (ELISpot) with frequencies that were severalfold higher than those detected using the [51Cr]-release assay. Interestingly, the effector cells were confined to the CD45RO1CD28 subset, implying that these cells are continuously derived from a resting memory population and are insensitive to costimulation by APC and thus are possibly prone to apoptosis once they have carried out their functions.76 In combination, these results suggest that in some subjects subclinical HCV infection leads to establishment of immunological memory. The likely corollary of this finding is that maintenance of such T-cell responses requires repeated low-level stimulation induced by unapparent infections or prolonged retention of viral Ag in lymph nodes or elsewhere.76 Another study examined the sexual partners of 52 healthcare workers who developed HCV infection as a result of a needlestick injury. These individuals were prospectively followed for 48 weeks after their partners exposure.79 Viraemia with seroconversion was detected in 8 of 54 (15%) sexual partners, of whom 4 (50%) went on to develop chronic HCV infection. Of 44 partners without viraemia or antibody production, 14 (32%) had detectable HCV-specific cellular immune responses to recombinant proteins in a lymphocyte proliferation assay (LPA) and an IFN-g ELISpot assay. The responses were of a significantly lower magnitude and breadth than those detected in individuals who had cleared the virus, but of higher magnitude and more diverse than those individuals with chronic disease. An ELISpot assay using purified CD81 cells and HLA-A2 restricted peptides was used to assess CTL activity in A2-positive subjects. At week 48, positive responses were detected in 12 of 13 (92%) individuals with resolved infection, in 5 of 8 (63%) antibody and PCRnegative subjects, and in 4 of 13 (31%) chronically infected individuals. The HCV immunity associated with the sexual route of exposure in this report may indicate that inoculation via the mucosal route or in low dosage may preferentially promote effective immunity. This possibility is further supported by a study of babies born to HCV-infected mothers. Twenty of 28 (71%) HCV PCR-negative babies born to HCV PCR-positive mothers had proliferative responses to 38 core, E1 and NS3 peptides in a 5bromodeoxyuridine incorporation assay.80 Infants responded to a greater number of peptides, and had responses of a higher
magnitude, than their chronically infected mothers. In addition, HCV-specific cellular immune responses were also found in 13 of 127 (18%) seronegative individuals living with a chronically infected family member.81 IFN-g ELISpot responses based predominantly on CD41 T cells were detected using pools of overlapping peptides covering the core and NS3NS5b regions. Interestingly, the majority of those with responses were children of HCV-positive parents (12/13). It may be that the majority of exposed HCV PCR-negative children develop HCV-specific cellular immune responses early in life, with the frequency of these responses declining over the following decades. Studies of IDU who are likely to have been exposed to multiple HCV variants as a result of repeated sharing of contaminated injecting apparatus provide the strongest, but still circumstantial, evidence for the protective nature of these cellular immune responses. Considering the high prevalence and incidence of HCV infection among IDU82,83 and the fact that most IDU become infected within the first 23 years of initiation into injecting drug use,84 it is likely that seronegative individuals from such groups will provide key insights into potentially protective immune responses. For instance, in a cohort of 782 individuals who had been injecting drugs for more than 10 years, a small subgroup of 46 individuals (5.9%) were identified who remained seronegative, despite the fact that 12 of these 46 individuals (26%) reported injecting daily, with the majority reporting high-risk injecting practices such as injecting cocaine (n = 36; 78%) and using a shooting gallery (n = 11; 22%) in the last 6 months.85 Despite being HCV seronegative, this subgroup showed evidence of exposure to other bloodborne viruses, including hepatitis B in 29 of the 46 individuals (62%) and HIV in 11 (22%). When compared with the majority of this cohort who were HCV seropositive, the seronegative minority reported similar levels of high-risk behaviour, indicating that, at least on the basis of probabilities, some of the persistently seronegative individuals were likely to have been previously exposed to HCV. Interestingly, subsequent studies of eight individuals from this group found no evidence of HCV-specific cellular immune responses, using a recombinant vacciniaHCV CTL assay.86 In contrast, we have recently reported analysis of HCV-specific immune responses in a cohort of 38 high-risk, seronegative IDU who reported a median of 7 years of injecting drug use, with 20 episodes of injecting per month, and of whom approximately half reported sharing of injecting apparatus and half had serological markers of natural exposure to HBV.77 Effector CD81 Tcell responses were detected by HCVvaccinia-based, IFN-g ELISpot assays in 22 of 29 (76%) HCV seronegative subjects. Positive responses were associated with higher risk behaviour (P = 0.04). Despite negative anti-HCV ELISA results, 33 of 36 (92%) subjects showed faint bands against HCV NS proteins (NS3, NS4 and/or NS5) on recombinant immunoblot analysis. In 4 of 36 subjects (11%), these bands met the manufacturers criteria for a positive result, whereas results were indeterminate for 29 of 36 (81%) subjects. Given the behavioural profile of these subjects, the immune responses described are likely to have been primed and maintained by episodes of subclinical infection without classical seroconversion and may indicate a phenotype that is resistant to establishment of chronic HCV infection.
2006 The Authors. Journal compilation 2006 Australasian Society for Immunology Inc.
Immunity against hepatitis C virus
243
Infection without seroconversion
Direct evidence for such a phenotype has recently been reported in both chimpanzees and humans. Transient viraemia and HCV-specific cellular immune responses were detected in two chimpanzees following sequential exposure to increasing infective HCV doses starting as low as one RNA (1) virion.87 Neither chimpanzee was anti-HCV positive after the initial infection with an estimated single virion; however, cellular immune responses were detected in PBMC both directly ex vivo and after expansion using a recombinant vacciniaHCV ELISpot assay. Comparable responses were also detected in intrahepatic lymphocytes after exposure to 1 or 10 RNA (1) virions. Increasing the dose to 100 RNA (1) virions induced both viraemia and seroconversion. This situation may be analogous to that studied in several experimental models, in which repeated or prolonged exposure to low levels of Ag has been shown to select for high-avidity T cells.8890 High-avidity T cells are associated with improved viral clearance rates in these models,91,92 which relates to the ability to initiate lysis of infected cells earlier in infection while Ag densities are low.93 In contrast, chimpanzees exposed to higher doses of virus may require both antibody and cellular immune responses for effective immune control. We have recently reported four cases of transient HCV viraemia with subsequent clearance, but without biochemical hepatitis or anti-HCV seroconversion, from a prospective cohort study of seronegative prison inmates. Subjects were screened monthly for incident infections and followed weekly from the onset of viraemia.78 After 26 months of viraemia, the subjects cleared HCV-RNA from the serum, but failed to develop anti-HCV antibodies over prolonged follow up. HCV-specific LPA and CTL responses were detected in both of the subjects who were assessed, with production of IFN-g in response to recombinant vacciniaHCV constructs also found in one. All subjects had risk factors for HCV transmission and despite repeatedly nonreactive HCV antibody ELISA results, all had weak, but consistent, serological reactivity against HCV NS proteins on immunoblot testing, including testing of stored samples collected well before the onset of viraemia. There have been previous reports of individuals who remained persistently viraemic without generating antibody responses, but these reports are limited by the use of first or second generation anti-HCV ELISA assays, which are likely to have reduced sensitivity.9497 Other reports of HIV coinfected individuals or subjects with hypogammaglobulinaemia have little relevance given the immunocompromised state.71,73 As these latter conditions were not present in the subjects in the prison study, these findings verify the occurrence of HCV infection in the absence of seroconversion in humans, and also support the evidence for the role of cellular immunity in facilitating clearance. In addition, given the high-risk profile of the inmates, the setting in which these cases occurred and the evidence for pre-existing immunity, these cases point to the likelihood that the episodes were of reinfection and to the existence of protective immunity that facilitated efficient viral clearance.
viduals who are exposed to HIV, but remain uninfected. Studies of such high-risk HIV seronegative subjects have identified HIV-specific cellular immune responses in uninfected babies born to infected mothers,98 health-care workers with occupational exposure99 and partners of HIV-positive individuals.100 The strongest evidence for protective immunity against HIV comes from sex workers in Nairobi who engaged in unprotected sex with clientele with a very high prevalence of HIV infection. These women were likely to have been exposed to numerous HIV variants, yet remained consistently uninfected.22,23 It has been hypothesized that these women may have received a low initial viral inoculum that efficiently primed a cell-mediated immune response in the absence of antibody synthesis.101 A diverse array of immune response characteristics have been implicated in this protective immunity, including a polarized Th1-cell response,102104 specific MHC class I and II alleles,105,106 CTL responses to envelope proteins and conserved peptide epitopes,100,107109 mucosal specific anti-HIV IgA production110,111 as well decreased expression of the chemokine co-receptors for viral entry, CXCR4 and CCR5.112,113 In addition, as several of these exposed, uninfected women were related, it is plausible that as yet unidentified genetic factors may have played a role.114 These immune responses may have been the result of HIV infection, but with extremely low levels of replication, as some individuals had HIV proviral DNA in resting CD41 cells at levels 104- to 106-fold lower than those in infected individuals well below the detection levels of conventional assays.115 Importantly, a number of these seronegative immune women have subsequently become infected with HIV following a period of reduction in frequency of, or an interruption to, sex work, suggesting that the protective mechanisms were maintained by repeated exposure to HIV.116 In many respects, HIV infection shares similar immunopathogenic mechanisms with HCV infection, as cellular immune responses are believed to be critical to the control of viral replication in both cases, but the viruses feature high levels of viral mutation allowing the development of escape mutants to subvert effective immune control. However, it should be noted that despite these similarities, HCV is not known to incorporate into the host genome. In addition, the viruses are generally transmitted via different routes, and hence do not generate identical patterns of immune response. HIV infection most commonly occurs via the genital mucosa and elicits CTL responses specific to mucosal virus.117 In contrast, HCV infection, which is almost exclusively transmitted from blood to blood, is associated with systemic CTL responses in the absence of mucosal CTL.118
Generation and maintenance of protective responses
It is well established in experimental systems that cross-reactivity in T-cell responses directed against two unrelated viruses can influence the generation of both the effector and memory T-cell populations. Lymphocytic choriomeningitis virus, Pichinde virus and vaccinia virus are recognized to have such cross-reactive epitopes, so that animals challenged with one virus have a rapid increase in cross-reactive clones when challenged with a second, unrelated virus.119 The initial antiviral responses appear to prime the immune system and increase clearance rates after subsequent infection with the unrelated, but crossreactive, virus.120 The phenomenon appears to be dependent
Analogy with HIV seronegative immune subjects
Cell mediated immune responses in viraemic, seronegative prisoners may well be comparable to those identified in rare indi-
2006 The Authors. Journal compilation 2006 Australasian Society for Immunology Inc.
244
LN Elliott et al.
on selective reactivation of memory T cells with specificities to the earlier infection.121 These findings may be relevant to HCV, given that a cross-reactive epitope is shared between the influenza virus and the NS3 protein of HCV,122 and CD81 T cells specific for this epitope have been found in patients with acute HCV.123 In the dose-escalating reinfection study with two chimpanzees, one animal with pre-existing NS3-specific responses went on to clear the virus, whereas the other became chronically infected.87 Thus, it is plausible that individuals who have strong pre-existing responses to the crossreactive epitopes derived from influenza, or other Ag, are able to mount a more rapid and effective immune response when subsequently exposed to HCV. It is plausible that these individuals with protective immunity were able to generate an immune response directed against a critical region of the HCV genome, resulting in an increased ability to clear the virus. Studies of seronegative immune individuals have predominantly used a small set of selected Ag; hence, a comprehensive study of the specificity of these responses is needed (Table 1). However, given that no significant difference has been found between the specificity of cellular immune responses in individuals with self-limiting disease and that of individuals with chronic infection, it appears unlikely that responses directed against particular epitopes are the only mechanism responsible for protective immunity.124 Recent experimental data indicate that CD81 responses can be generated from uninfected cells, thus calling into question the dogma that the class I pathway is available only to replicating Ag. Dendritic cells are able to present Ag derived by phagocytosis of infected cells that have undergone apoptosis, thereby eliciting Ag-specific CD81 immune responses.125 This pathway may provide a mechanism by which individuals can be exposed to predominantly non-infectious HCV particles and generate HCV-specific responses without substantive viral replication being established. As an in vitro culture system to support HCV replication has only very recently been reported, very little is known about the propensity for HCV to produce defective virions. However, the key enzyme involved in replication of the virus, the RNAdependent RNA polymerase, has no proof-reading activity
Table 1 HCV-specific cellular immune responses in seronegative cohorts Risk factor for HCV exposure Spouses of chronically infected individuals74 Health-care workers75 Family members of chronically infected individuals76 Spouses of chronically infected individuals79 IDU77 IDU78 Spouses of chronically infected individuals81 Infants born to HCV PCR-positive mothers80 Assay and Ag used
and poor fidelity, with a calculated mutation rate of between 0.4 103 and 1.92 103 base substitutions per genome site per year.126 This is comparable to the mutation rate in HIV reverse transcriptase of between 103 and 104 substitutions per site.127 Thus, there is a high likelihood that defective virions are indeed produced during HCV replication in vivo. The role of ongoing Ag exposure in the maintenance of Agspecific cellular immune responses remains unresolved. It was initially argued that memory cells were only maintained by contact with trace amounts of specific Ag that remained after primary exposure.128 Several authors subsequently showed that both CD81 and CD41 memory T cells can survive in the absence of Ag.129131 However, there remains some dispute as to whether experimental evidence for Ag-independent T-cell memory provides a valid model of T-cell memory within a functioning immune system.132 It is therefore unclear whether the maintenance of HCV-specific T cells following viral clearance, or of those found in seronegative, immune individuals, requires repeated exposure to HCV Ag. The report that established HIV infection in seronegative immune sex workers may follow from a break in sex work suggests that regular Ag exposure is required to maintain HIV-specific cellular immune responses. It is plausible that a reservoir of infected cells with extremely low levels of HCV replication could remain protected from the immune system, such as within the liver, dendritic cells, PBMC or the brain.133138 Extrahepatic replication of HCV can occur in the lymph nodes, pancreas and, to a lesser extent, spleen, adrenal gland, bone marrow and thyroid tissue of patients coinfected with HIV; however, it remains unclear if this occurs in patients infected with HCV alone.139141 Importantly, recent studies using ultrasensitive PCR assays for HCV negative strand intermediates to screen patients who had previously cleared infection or had been successfully treated have shown that a significant proportion appear to harbour very low levels of residual virus in PBMC, but not in the liver.142,143 A more detailed understanding of the generation and maintenance of HCV-specific cellular immune responses in these seronegative immune individuals may provide key insights into the most appropriate directions for vaccine design. Future
No. subjects with HCV-specific cellular immune responses 4/20 2/11 7/29 14/44 22/29 two individuals 13/71 20/28
LPA: core, NS3-4, NS4 and NS5 proteins CTL and LPA: 10 core, E1 and NS3 peptides LPA: core, E1, E2, NS3, NS4 and NS5 proteins ELISpot and CTL: 20 core, E1, E2, NS3, NS4 and NS5 peptides LPA and ELISpot: core, NS3, NS4 and NS5 proteins ELISpot: 18 core, E1 and NS4 peptides ELISpot: coreNS2 and NS2-5 recombinant vaccinia virus constructs ELISpot and CTL: coreNS2 and NS2-5 recombinant vaccinia virus constructs LPA: core, NS3-4, NS4 and NS5 proteins ELISpot: 216 overlapping peptides covering core and NS3-NS5b BrdU incorporation: 38 core, E1 and NS3 peptides
BrdU, 5-bromodeoxyuridine; ELISpot, enzyme-linked immunospot assay; HCV, hepatitis C virus; IDU, injecting drug users; LPA, lymphocyte proliferation assay; NS, nonstructural.
2006 The Authors. Journal compilation 2006 Australasian Society for Immunology Inc.
Immunity against hepatitis C virus
245
studies should focus on the contributions that high-avidity T cells and dominant protective epitopes play in the seronegative immune phenotype. In addition, the role of other host factors, including genetic polymorphisms and behavioural patterns in the setting of first exposure, as well as viral factors requires further study. This information may aid in the development of a vaccine that mimics the protective immune responses seen in these individuals without the need for repeated Ag exposure.
Conclusion
The combined evidence from these studies indicates that in some individuals, strong initial HCV-specific cellular immune responses are able to prevent the establishment of chronic HCV infection. In a small subset of cases, this immune response may confer the capacity to rapidly clear the virus after repeated exposures to multiple HCV genotypes without seroconversion. This protection against chronic infection is primarily mediated through HCV-specific cellular immune responses, indicating that this should be an important focus of vaccine design. Although successful clearance can occur without an antibody response, it remains unclear if the generation of antibodies, particularly neutralizing antibodies, would increase the effectiveness of vaccine candidates. Given the global burden of HCV disease, an understanding of how protective immune responses are generated is critical. Studies of subjects who fall into this unique group may provide key insights into the nature of these protective immune responses and guide vaccine development and immunotherapeutic options.
Acknowledgements
We would like to thank Professor Richard Strugnell and Associate Professor David Anderson for critical review of this article.
References
1 Fujinami RS, Oldstone MB. Antiviral antibody reacting on the plasma membrane alters measles virus expression inside the cell. Nature 1979; 279: 52930. 2 Oldstone MB, Fujinami RS, Lampert PW. Membrane and cytoplasmic changes in virus-infected cells induced by interactions of antiviral antibody with surface viral antigen. Prog. Med. Virol. 1980; 26: 4593. 3 Reinhardt B, Jaspert R, Niedrig M, Kostner C, L Age-Stehr J. Development of viremia and humoral and cellular parameters of immune activation after vaccination with yellow fever virus strain 17D: a model of human flavivirus infection. J. Med. Virol. 1998; 56: 15967. 4 Law M, Smith GL. Antibody neutralization of the extracellular enveloped form of vaccinia virus. Virology 2001; 280: 13242. 5 Flamand A, Raux H, Gaudin Y, Ruigrok RW. Mechanisms of rabies virus neutralization. Virology 1993; 194: 30213. 6 Pantaleo G, Demarest JF, Vaccarezza M et al. Effect of anti-V3 antibodies on cell-free and cell-to-cell human immunodeficiency virus transmission. Eur. J. Immunol. 1995; 25: 22631. 7 Burioni R, Williamson RA, Sanna PP, Bloom FE, Burton DR. Recombinant human Fab to glycoprotein D neutralizes infectivity and prevents cell-to-cell transmission of herpes simplex viruses 1 and 2 in vitro. Proc. Natl Acad. Sci. USA 1994; 91: 3559.
8 Burton DR, Williamson RA, Parren PW. Antibody and virus: binding and neutralization. Virology 2000; 270: 13. 9 Klasse PJ, Sattentau QJ. Occupancy and mechanism in antibody-mediated neutralization of animal viruses. J. Gen. Virol. 2002; 83: 2091108. 10 Alter H. Discovery of non-A, non-B hepatitis and identification of its etiology. Am. J. Med. 1999; 107: 1620. 11 Gerlach JT, Diepolder HM, Zachoval R et al. Acute hepatitis C: high rate of both spontaneous and treatment-induced viral clearance. Gastroenterology 2003; 125: 8088. 12 Freeman AJ, Marinos G, Ffrench RA, Lloyd AR. Immunopathogenesis of hepatitis C virus infection. Immunol. Cell Biol. 2001; 79: 51536. 13 Thomas DL, Astemborski J, Rai RM et al. The natural history of hepatitis C virus infection: host, viral, and environmental factors. JAMA 2000; 284: 45056. 14 Seeff LB. Natural history of chronic hepatitis C. Hepatology 2002; 36: S35S46. 15 Santantonio T, Sinisi E, Guastadisegni A et al. Natural course of acute hepatitis C: a long-term prospective study. Dig. Liver Dis. 2003; 35: 10413. 16 Kenny-Walsh E. Clinical outcomes after hepatitis C infection from contaminated anti-D immune globulin. Irish Hepatology Research Group. N. Engl. J. Med. 1999; 340: 122833. 17 Lai ME, Mazzoleni AP, Argiolu F et al. Hepatitis C virus in multiple episodes of acute hepatitis in polytransfused thalassaemic children. Lancet 1994; 343: 38890. 18 Farci P, Alter HJ, Govindarajan S et al. Lack of protective immunity against reinfection with hepatitis C virus. Science 1992; 258: 13540. 19 Bassett SE, Guerra B, Brasky K et al. Protective immune response to hepatitis C virus in chimpanzees rechallenged following clearance of primary infection. Hepatology 2001; 33: 147987. 20 Major ME, Mihalik K, Puig M et al. Previously infected and recovered chimpanzees exhibit rapid responses that control hepatitis C virus replication upon rechallenge. J. Virol. 2002; 76: 658695. 21 Prince AM, Brotman B, Huima T, Pascual D, Jaffery M, Inchauspe G. Immunity in hepatitis C infection. J. Infect. Dis. 1992; 165: 43843. 22 Rowland-Jones S, Sutton J, Ariyoshi K et al. HIV-specific cytotoxic T-cells in HIV-exposed but uninfected Gambian women. Nat. Med. 1995; 1: 5964. 23 Fowke KR, Nagelkerke NJ, Kimani J et al. Resistance to HIV1 infection among persistently seronegative prostitutes in Nairobi, Kenya. Lancet 1996; 348: 134751. 24 Bassett SE, Brasky KM, Lanford RE. Analysis of hepatitis C virus-inoculated chimpanzees reveals unexpected clinical profiles. J. Virol. 1998; 72: 258999. 25 Pancholi P, Lee DH, Liu Q et al. DNA prime/canarypox boostbased immunotherapy of chronic hepatitis B virus infection in a chimpanzee. Hepatology 2001; 33: 44854. 26 Kolykhalov AA, Agapov EV, Blight KJ, Mihalik K, Feinstone SM, Rice CM. Transmission of hepatitis C by intrahepatic inoculation with transcribed RNA. Science 1997; 277: 57074. 27 Chen M, Sallberg M, Sonnerborg A et al. Limited humoral immunity in hepatitis C virus infection. Gastroenterology 1999; 116: 13543. 28 Takaki A, Wiese M, Maertens G et al. Cellular immune responses persist and humoral responses decrease two decades after recovery from a single-source outbreak of hepatitis C. Nat. Med. 2000; 6: 57882.
2006 The Authors. Journal compilation 2006 Australasian Society for Immunology Inc.
246
LN Elliott et al.
29 Villano SA, Vlahov D, Nelson KE, Cohn S, Thomas DL. Persistence of viremia and the importance of long-term follow-up after acute hepatitis C infection. Hepatology 1999; 29: 90814. 30 Abe K, Inchauspe G, Shikata T, Prince AM. Three different patterns of hepatitis C virus infection in chimpanzees. Hepatology 1992; 15: 69095. 31 Farci P, Shimoda A, Wong D et al. Prevention of hepatitis C virus infection in chimpanzees by hyperimmune serum against the hypervariable region 1 of the envelope 2 protein. Proc. Natl Acad. Sci. USA 1996; 93: 15 3949. 32 Mehta SH, Cox A, Hoover DR et al. Protection against persistence of hepatitis C. Lancet 2002; 359: 147883. 33 Bjoro K, Froland SS, Yun Z, Samdal HH, Haaland T. Hepatitis C infection in patients with primary hypogammaglobulinemia after treatment with contaminated immune globulin. N. Engl. J. Med. 1994; 331: 160711. 34 Razvi S, Schneider L, Jonas MM, Cunningham-Rundles C. Outcome of intravenous immunoglobulin-transmitted hepatitis C virus infection in primary immunodeficiency. Clin. Immunol. 2001; 101: 2848. 35 Chapel HM, Christie JM, Peach V, Chapman RW. Five-year follow-up of patients with primary antibody deficiencies following an outbreak of acute hepatitis C. Clin. Immunol. 2001; 99: 32024. 36 Kobayashi M, Tanaka E, Matsumoto A, Ichijo T, Kiyosawa K. Antibody response to E2/NS1 hepatitis C virus protein in patients with acute hepatitis C. J. Gastroenterol. Hepatol. 1997; 12: 736. 37 Grellier L, Brown D, Power J, Dusheiko G. Absence of antienvelope antibodies and clearance of hepatitis C virus in a cohort of Irish women infected in 1977. J. Viral Hepat. 1997; 4: 37981. 38 Logvinoff C, Major ME, Oldach D et al. Neutralizing antibody response during acute and chronic hepatitis C virus infection. Proc. Natl Acad. Sci. USA 2004; 101: 10 14954. 39 Yu MY, Bartosch B, Zhang P et al. Neutralizing antibodies to hepatitis C virus (HCV) in immune globulins derived from anti-HCV-positive plasma. Proc. Natl Acad. Sci. USA 2004; 101: 7705710. 40 Farci P, Alter HJ, Wong DC et al. Prevention of hepatitis C virus infection in chimpanzees after antibody-mediated in vitro neutralization. Proc. Natl Acad. Sci. USA 1994; 91: 77926. 41 Bartosch B, Bukh J, Meunier JC et al. In vitro assay for neutralizing antibody to hepatitis C virus: evidence for broadly conserved neutralization epitopes. Proc. Natl Acad. Sci. USA 2003; 100: 14 199204. 42 Lavillette D, Morice Y, Germanidis G et al. Human serum facilitates hepatitis C virus infection, and neutralizing responses inversely correlate with viral replication kinetics at the acute phase of hepatitis C virus infection. J. Virol. 2005; 79: 602334. 43 Scarselli E, Cerino A, Esposito G, Silini E, Mondelli MU, Traboni C. Occurrence of antibodies reactive with more than one variant of the putative envelope glycoprotein (gp70) hypervariable region 1 in viremic hepatitis C virus-infected patients. J. Virol. 1995; 69: 440712. 44 Shimizu YK, Hijikata M, Iwamoto A, Alter HJ, Purcell RH, Yoshikura H. Neutralizing antibodies against hepatitis C virus and the emergence of neutralization escape mutant viruses. J. Virol. 1994; 68: 1494500. 45 Lechner F, Wong DK, Dunbar PR et al. Analysis of successful immune responses in persons infected with hepatitis C virus. J. Exp. Med. 2000; 191: 1499512.
46 Thimme R, Bukh J, Spangenberg HC et al. Viral and immunological determinants of hepatitis C virus clearance, persistence, and disease. Proc. Natl Acad. Sci. USA 2002; 99: 15 6618. 47 Gerlach JT, Diepolder HM, Jung MC et al. Recurrence of hepatitis C virus after loss of virus-specific CD4(1) T-cell response in acute hepatitis C. Gastroenterology 1999; 117: 93341. 48 Wertheimer AM, Miner C, Lewinsohn DM, Sasaki AW, Kaufman E, Rosen HR. Novel CD41 and CD81 T-cell determinants within the NS3 protein in subjects with spontaneously resolved HCV infection. Hepatology 2003; 37: 57789. 49 Lauer GM, Barnes E, Lucas M et al. High resolution analysis of cellular immune responses in resolved and persistent hepatitis C virus infection. Gastroenterology 2004; 127: 92436. 50 Chang KM, Thimme R, Melpolder JJ et al. Differential CD41 and CD81 T-cell responsiveness in hepatitis C virus infection. Hepatology 2001; 33: 26776. 51 Tsai SL, Liaw YF, Chen MH, Huang CY, Kuo GC. Detection of type 2-like T-helper cells in hepatitis C virus infection: implications for hepatitis C virus chronicity. Hepatology 1997; 25: 44958. 52 Diepolder HM, Zachoval R, Hoffmann RM et al. Possible mechanism involving T-lymphocyte response to non-structural protein 3 in viral clearance in acute hepatitis C virus infection. Lancet 1995; 346: 10061007. 53 Cooper S, Erickson AL, Adams EJ et al. Analysis of a successful immune response against hepatitis C virus. Immunity 1999; 10: 43949. 54 Gruner NH, Gerlach TJ, Jung MC et al. Association of hepatitis C virus-specific CD81 T cells with viral clearance in acute hepatitis C. J. Infect. Dis. 2000; 181: 152836. 55 Cucchiarini M, Kammer AR, Grabschield B et al. Vigorous peripheral blood cytotoxic T cell response during the acute phase of hepatitis C virus infection. Cell. Immunol. 2000; 203: 11123. 56 Nelson DR, Marousis CG, Davis GL et al. The role of hepatitis C virus-specific cytotoxic T lymphocytes in chronic hepatitis C. J. Immunol. 1997; 158: 147381. 57 Freeman AJ, Pan Y, Harvey CE et al. The presence of an intrahepatic cytotoxic T lymphocyte response is associated with low viral load in patients with chronic hepatitis C virus infection. J. Hepatol. 2003; 38: 34956. 58 Shoukry NH, Grakoui A, Houghton M et al. Memory CD81 T cells are required for protection from persistent hepatitis C virus infection. J. Exp. Med. 2003; 197: 164555. 59 Thimme R, Oldach D, Chang KM, Steiger C, Ray SC, Chisari FV . Determinants of viral clearance and persistence during acute hepatitis C virus infection. J. Exp. Med. 2001; 194: 1395406. 60 Ulsenheimer A, Gerlach JT, Gruener NH et al. Detection of functionally altered hepatitis C virus-specific CD4 T cells in acute and chronic hepatitis C. Hepatology 2003; 37: 118998. 61 Gruener NH, Lechner F, Jung MC et al. Sustained dysfunction of antiviral CD81 T lymphocytes after infection with hepatitis C virus. J. Virol. 2001; 75: 555058. 62 Thursz M, Yallop R, Goldin R, Trepo C, Thomas HC. Influence of MHC class II genotype on outcome of infection with hepatitis C virus. Lancet 1999; 354: 211924. 63 Cramp ME, Carucci P, Underhill J, Naoumov NV, Williams R, Donaldson PT. Association between HLA class II genotype and spontaneous clearance of hepatitis C viraemia. J. Hepatol. 1998; 29: 20713.
2006 The Authors. Journal compilation 2006 Australasian Society for Immunology Inc.
Immunity against hepatitis C virus
247
64 Zavaglia C, Martinetti M, Silini E et al. Association between HLA class II alleles and protection from or susceptibility to chronic hepatitis C. J. Hepatol. 1998; 28: 17. 65 Harcourt G, Hellier S, Bunce M et al. Effect of HLA class II genotype on T helper lymphocyte responses and viral control in hepatitis C virus infection. J. Viral Hepat. 2001; 8: 1749. 66 Chang KM, Rehermann B, McHutchison JG et al. Immunological significance of cytotoxic T lymphocyte epitope variants in patients chronically infected by the hepatitis C virus. J. Clin. Invest. 1997; 100: 237685. 67 Nascimbeni M, Mizukoshi E, Bosmann M et al. Kinetics of CD41 and CD81 memory T-cell responses during hepatitis C virus rechallenge of previously recovered chimpanzees. J. Virol. 2003; 77: 478193. 68 Grakoui A, Shoukry NH, Woollard DJ et al. HCV persistence and immune evasion in the absence of memory T cell help. Science 2003; 302: 65962. 69 Micallef JM, Jauncey M, Amin J et al. Hepatitis C virus reinfection within a cohort of injecting drug users. Hepatology 2003; 38: 266A. 70 Wiese M, Berr F, Lafrenz M, Porst H, Oesen U. Low frequency of cirrhosis in a hepatitis C (genotype 1b) singlesource outbreak in Germany: a 20-year multicenter study. Hepatology 2000; 32: 916. 71 George SL, Gebhardt J, Klinzman D et al. Hepatitis C virus viremia in HIV-infected individuals with negative HCV antibody tests. J. Acquir. Immune Defic. Syndr. 2002; 31: 15462. 72 Thio CL, Nolt KR, Astemborski J, Vlahov D, Nelson KE, Thomas DL. Screening for hepatitis C virus in human immunodeficiency virus-infected individuals. J. Clin. Microbiol. 2000; 38: 5757. 73 Rossi G, Tucci A, Cariani E, Ravaggi A, Rossini A, Radaeli E. Outbreak of hepatitis C virus infection in patients with hematologic disorders treated with intravenous immunoglobulins: different prognosis according to the immune status. Blood 1997; 90: 130914. 74 Bronowicki JP, Vetter D, Uhl G et al. Lymphocyte reactivity to hepatitis C virus (HCV) antigens shows evidence for exposure to HCV in HCV-seronegative spouses of HCV-infected patients. J. Infect. Dis. 1997; 176: 51822. 75 Koziel MJ, Wong DK, Dudley D, Houghton M, Walker BD. Hepatitis C virus-specific cytolytic T lymphocyte and T helper cell responses in seronegative persons. J. Infect. Dis. 1997; 176: 85966. 76 Scognamiglio P, Accapezzato D, Casciaro MA et al. Presence of effector CD81 T cells in hepatitis C virus-exposed healthy seronegative donors. J. Immunol. 1999; 162: 66819. 77 Freeman AJ, Ffrench RA, Post JJ et al. Prevalence of production of virus-specific interferon-gamma among seronegative hepatitis C-resistant subjects reporting injection drug use. J. Infect. Dis. 2004; 190: 10937. 78 Post JJ, Pan Y, Freeman AJ et al. Clearance of hepatitis C viremia associated with cellular immunity in the absence of seroconversion in the hepatitis C incidence and transmission in prisons study cohort. J. Infect. Dis. 2004; 189: 184655. 79 Kamal SM, Amin A, Madwar M et al. Cellular immune responses in seronegative sexual contacts of acute hepatitis C patients. J. Virol. 2004; 78: 12 2528. 80 Della Bella S, Riva A, Tanzi E et al. Hepatitis C virus-specific reactivity of CD41-lymphocytes in children born from HCVinfected women. J. Hepatol. 2005; 43: 394402.
81 Al-Sherbiny M, Osman A, Mohamed N et al. Exposure to hepatitis C virus induces cellular immune responses without detectable viremia or seroconversion. Am. J. Trop. Med. Hyg. 2005; 73: 449. 82 Crofts N, Jolley D, Kaldor J, van Beek I, Wodak A. Epidemiology of hepatitis C virus infection among injecting drug users in Australia. J. Epidemiol. Community Health 1997; 51: 6927. 83 Villano SA, Vlahov D, Nelson KE, Lyles CM, Cohn S, Thomas DL. Incidence and risk factors for hepatitis C among injection drug users in Baltimore, Maryland. J. Clin. Microbiol. 1997; 35: 32747. 84 van Beek I, Dwyer R, Dore GJ, Luo K, Kaldor JM. Infection with HIV and hepatitis C virus among injecting drug users in a prevention setting: retrospective cohort study. BMJ 1998; 317: 4337. 85 Thomas DL, Vlahov D, Solomon L et al. Correlates of hepatitis C virus infections among injection drug users. Medicine (Baltimore) 1995; 74: 21220. 86 Wong DK, Dudley DD, Dohrenwend PB et al. Detection of diverse hepatitis C virus (HCV)-specific cytotoxic T lymphocytes in peripheral blood of infected persons by screening for responses to all translated proteins of HCV . J. Virol. 2001; 75:122935. 87 Shata MT, Tricoche N, Perkus M et al. Exposure to low infective doses of HCV induces cellular immune responses without consistently detectable viremia or seroconversion in chimpanzees. Virology 2003; 314: 60116. 88 Cai Z, Sprent J. Influence of antigen dose and costimulation on the primary response of CD81 T cells in vitro. J. Exp. Med. 1996; 183: 224757. 89 Rees W, Bender J, Teague TK et al. An inverse relationship between T cell receptor affinity and antigen dose during CD4(1) T cell responses in vivo and in vitro. Proc. Natl Acad. Sci. USA 1999; 96: 97816. 90 Oh S, Hodge JW, Ahlers JD, Burke DS, Schlom J, Berzofsky JA. Selective induction of high avidity CTL by altering the balance of signals from APC. J. Immunol. 2003; 170: 252330. 91 Gallimore A, Dumrese T, Hengartner H, Zinkernagel RM, Rammensee HG. Protective immunity does not correlate with the hierarchy of virus-specific cytotoxic T cell responses to naturally processed peptides. J. Exp. Med. 1998; 187: 1647 57. 92 Slifka MK, Whitton JL. Functional avidity maturation of CD8(1) T cells without selection of higher affinity TCR. Nat. Immunol. 2001; 2: 71117. 93 Derby M, Alexander-Miller M, Tse R, Berzofsky J. Highavidity CTL exploit two complementary mechanisms to provide better protection against viral infection than low-avidity CTL. J. Immunol. 2001; 166: 169097. 94 Beld M, Penning M, van Putten M et al. Low levels of hepatitis C virus RNA in serum, plasma, and peripheral blood mononuclear cells of injecting drug users during long antibodyundetectable periods before seroconversion. Blood 1999; 94: 118391. 95 Durand F, Danic B, Tardivel R et al. Discovery of a chronic HVC infection without seroconversion in a blood donor in France during 28 months. Transfus. Clin. Biol. 2000; 7: 24250. 96 Durand F, Beauplet A, Marcellin P. Evidence of hepatitis C virus viremia without detectable antibody to hepatitis C virus in a blood donor. Ann. Intern. Med. 2000; 133: 745.
2006 The Authors. Journal compilation 2006 Australasian Society for Immunology Inc.
248
LN Elliott et al.
97 Peoples BG, Preston SB, Tzeng JL, Stramer SL, Gifford L, Wissel ME. Prolonged antibody-negative HCV viremia in a US blood donor with apparent HCV transmission to a recipient. Transfusion (Paris) 2000; 40: 128081. 98 Clerici M, Sison AV, Berzofsky JA et al. Cellular immune factors associated with mother-to-infant transmission of HIV. AIDS 1993; 7: 142733. 99 Clerici M, Levin JM, Kessler HA et al. HIV-specific T-helper activity in seronegative health care workers exposed to contaminated blood. JAMA 1994; 271: 426. 100 Langlade-Demoyen P, Ngo-Giang-Huong N, Ferchal F, Oksenhendler E. Human immunodeficiency virus (HIV) Nefspecific cytotoxic T lymphocytes in noninfected heterosexual contact of HIV-infected patients. J. Clin. Invest. 1994; 93: 12937. 101 Rowland-Jones SL, McMichael A. Immune responses in HIVexposed seronegatives: have they repelled the virus? Curr. Opin. Immunol. 1995; 7: 44855. 102 Fowke KR, Kaul R, Rosenthal KL et al. HIV-1-specific cellular immune responses among HIV-1-resistant sex workers. Immunol. Cell Biol. 2000; 78: 58695. 103 Clerici M, Giorgi JV , Chou CC et al. Cell-mediated immune response to human immunodeficiency virus (HIV) type 1 in seronegative homosexual men with recent sexual exposure to HIV-1. J. Infect. Dis. 1992; 165: 101219. 104 Pinto LA, Sullivan J, Berzofsky JA et al. ENV-specific cytotoxic T lymphocyte responses in HIV seronegative health care workers occupationally exposed to HIV-contaminated body fluids. J. Clin. Invest. 1995; 96: 86776. 105 MacDonald KS, Embree J, Njenga S et al. Mother-child class I HLA concordance increases perinatal human immunodeficiency virus type 1 transmission. J. Infect. Dis. 1998; 177: 5516. 106 MacDonald KS, Fowke KR, Kimani J et al. Influence of HLA supertypes on susceptibility and resistance to human immunodeficiency virus type 1 infection. J. Infect. Dis. 2000; 181: 15819. 107 Rowland-Jones SL, Nixon DF, Aldhous MC et al. HIV-specific cytotoxic T-cell activity in an HIV-exposed but uninfected infant. Lancet 1993; 341: 86061. 108 Rowland-Jones SL, Dong T, Fowke KR et al. Cytotoxic T cell responses to multiple conserved HIV epitopes in HIVresistant prostitutes in Nairobi. J. Clin. Invest. 1998; 102: 175865. 109 Kaul R, Rowland-Jones SL, Kimani J et al. New insights into HIV-1 specific cytotoxic T-lymphocyte responses in exposed, persistently seronegative Kenyan sex workers. Immunol. Lett. 2001; 79: 313. 110 Mazzoli S, Trabattoni D, Lo Caputo S et al. HIV-specific mucosal and cellular immunity in HIV-seronegative partners of HIV-seropositive individuals. Nat. Med. 1997; 3: 125057. 111 Kaul R, Trabattoni D, Bwayo JJ et al. HIV-1-specific mucosal IgA in a cohort of HIV-1-resistant Kenyan sex workers. AIDS 1999; 13: 239. 112 Jennes W, Sawadogo S, Koblavi-Deme S et al. Cellular human immunodeficiency virus (HIV)-protective factors: a comparison of HIV-exposed seronegative female sex workers and female blood donors in Abidjan, Cote dIvoire. J. Infect. Dis. 2003; 187: 20614. 113 Alvarez V, Lopez-Larrea C, Coto E. Mutational analysis of the CCR5 and CXCR4 genes (HIV-1 co-receptors) in resistance to HIV-1 infection and AIDS development among intravenous drug users. Hum. Genet. 1998; 102: 4836.
114 Plummer FA, Ball TB, Kimani J, Fowke KR. Resistance to HIV-1 infection among highly exposed sex workers in Nairobi: what mediates protection and why does it develop? Immunol. Lett. 1999; 66: 2734. 115 Zhu T, Corey L, Hwangbo Y et al. Persistence of extraordinarily low levels of genetically homogeneous human immunodeficiency virus type 1 in exposed seronegative individuals. J. Virol. 2003; 77: 610816. 116 Kaul R, Rowland-Jones SL, Kimani J et al. Late seroconversion in HIV-resistant Nairobi prostitutes despite pre-existing HIV-specific CD81 responses. J. Clin. Invest. 2001; 107: 3419. 117 Murphey-Corb M, Wilson LA, Trichel AM et al. Selective induction of protective MHC class I-restricted CTL in the intestinal lamina propria of rhesus monkeys by transient SIV infection of the colonic mucosa. J. Immunol. 1999; 162: 54049. 118 Belyakov IM, Ahlers JD, Brandwein BY et al. The importance of local mucosal HIV-specific CD8(1) cytotoxic T lymphocytes for resistance to mucosal viral transmission in mice and enhancement of resistance by local administration of IL-12. J. Clin. Invest. 1998; 102: 207281. 119 Selin LK, Nahill SR, Welsh RM. Cross-reactivities in memory cytotoxic T lymphocyte recognition of heterologous viruses. J. Exp. Med. 1994; 179: 193343. 120 Selin LK, Varga SM, Wong IC, Welsh RM. Protective heterologous antiviral immunity and enhanced immunopathogenesis mediated by memory T cell populations. J. Exp. Med. 1998; 188: 170515. 121 Selin LK, Lin MY, Kraemer KA et al. Attrition of T cell memory: selective loss of LCMV epitope-specific memory CD8 T cells following infections with heterologous viruses. Immunity 1999; 11: 73342. 122 Wedemeyer H, Mizukoshi E, Davis AR, Bennink JR, Rehermann B. Cross-reactivity between hepatitis C virus and influenza A virus determinant-specific cytotoxic T cells. J. Virol. 2001; 75: 11 392400. 123 Urbani S, Amadei B, Fisicaro P et al. Heterologous T cell immunity in severe hepatitis C virus infection. J. Exp. Med. 2005; 201: 67580. 124 Lauer GM, Ouchi K, Chung RT et al. Comprehensive analysis of CD8(1)-T-cell responses against hepatitis C virus reveals multiple unpredicted specificities. J. Virol. 2002; 76: 610413. 125 Albert ML, Sauter B, Bhardwaj N. Dendritic cells acquire antigen from apoptotic cells and induce class I-restricted CTLs. Nature 1998; 392: 869. 126 Ogata N, Alter HJ, Miller RH, Purcell RH. Nucleotide sequence and mutation rate of the H strain of hepatitis C virus. Proc. Natl Acad. Sci. USA 1991; 88: 33926. 127 Nowak M. HIV mutation rate. Nature 1990; 347: 522. 128 Zinkernagel RM, Bachmann MF, Kundig TM, Oehen S, Pirchet H, Hengartner H. On immunological memory. Annu. Rev. Immunol. 1996; 14: 33367. 129 Mullbacher A. The long-term maintenance of cytotoxic T cell memory does not require persistence of antigen. J. Exp. Med. 1994; 179: 31721. 130 Lau LL, Jamieson BD, Somasundaram T, Ahmed R. Cytotoxic T-cell memory without antigen. Nature 1994; 369: 64852. 131 Veiga-Fernandes H, Walter U, Bourgeois C, McLean A, Rocha B. Response of naive and memory CD81 T cells to antigen stimulation in vivo. Nat. Immunol. 2000; 1: 4753. 132 Zinkernagel RM. On differences between immunity and immunological memory. Curr. Opin. Immunol. 2002; 14: 52336.
2006 The Authors. Journal compilation 2006 Australasian Society for Immunology Inc.
Immunity against hepatitis C virus
249
133 Bronowicki JP, Loriot MA, Thiers V , Grignon Y, Zignego AL, Brechot C. Hepatitis C virus persistence in human hematopoietic cells injected into SCID mice. Hepatology 1998; 28: 21118. 134 Laporte J, Bain C, Maurel P, Inchauspe G, Agut H, Cahour A. Differential distribution and internal translation efficiency of hepatitis C virus quasispecies present in dendritic and liver cells. Blood 2003; 101: 527. 135 Crovatto M, Pozzato G, Zorat F et al. Peripheral blood neutrophils from hepatitis C virus-infected patients are replication sites of the virus. Haematologica 2000; 85: 35661. 136 Sansonno D, Lotesoriere C, Cornacchiulo V et al. Hepatitis C virus infection involves CD34(1) hematopoietic progenitor cells in hepatitis C virus chronic carriers. Blood 1998; 92: 332837. 137 Laskus T, Radkowski M, Bednarska A et al. Detection and analysis of hepatitis C virus sequences in cerebrospinal fluid. J. Virol. 2002; 76: 10 0648. 138 Radkowski M, Wilkinson J, Nowicki M et al. Search for hepatitis C virus negative-strand RNA sequences and analysis of viral sequences in the central nervous system: evidence of replication. J. Virol. 2002; 76: 600608.
139 Laskus T, Radkowski M, Wang LF, Vargas H, Rakela J. Search for hepatitis C virus extrahepatic replication sites in patients with acquired immunodeficiency syndrome: specific detection of negative-strand viral RNA in various tissues. Hepatology 1998; 28: 1398401. 140 Laskus T, Radkowski M, Wang LF, Jang SJ, Vargas H, Rakela J. Hepatitis C virus quasispecies in patients infected with HIV-1: correlation with extrahepatic viral replication. Virology 1998; 248: 16471. 141 Laskus T, Radkowski M, Wang LF, Nowicki M, Rakela J. Uneven distribution of hepatitis C virus quasispecies in tissues from subjects with end-stage liver disease: confounding effect of viral adsorption and mounting evidence for the presence of low-level extrahepatic replication. J. Virol. 2000; 74: 101417. 142 Pham TN, MacParland SA, Mulrooney PM, Cooksley H, Naoumov NV , Michalak TI. Hepatitis C virus persistence after spontaneous or treatment-induced resolution of hepatitis C. J. Virol. 2004; 78: 586774. 143 Radkowski M, Gallegos-Orozco JF, Jablonska J et al. Persistence of hepatitis C virus in patients successfully treated for chronic hepatitis C. Hepatology 2005; 41: 10614.
2006 The Authors. Journal compilation 2006 Australasian Society for Immunology Inc.
Вам также может понравиться
- HEP-Adaptive Immune ResponsesДокумент7 страницHEP-Adaptive Immune ResponsesoomculunОценок пока нет
- 2021 NATURE Neutralizing Antibody Titres in SARS-CoV-2Документ7 страниц2021 NATURE Neutralizing Antibody Titres in SARS-CoV-2Yuna SaspitaОценок пока нет
- Are COVID Vaccines Effective for Immunocompromised PeopleДокумент4 страницыAre COVID Vaccines Effective for Immunocompromised PeopleMARHUMA HAPSIN. ABBASОценок пока нет
- HBV HCV 1Документ13 страницHBV HCV 1Vũ Minh KhoaОценок пока нет
- ZJV 10786Документ16 страницZJV 10786runky febrankaОценок пока нет
- To Neutralize or Not, A Key HIV Vaccine Question: Between Bedside and BenchДокумент3 страницыTo Neutralize or Not, A Key HIV Vaccine Question: Between Bedside and Benchzee4600Оценок пока нет
- Cohen 2008Документ5 страницCohen 2008Dee SobriОценок пока нет
- Good Cop, Bad Cop? Interrogating The Immune Responses To Primate Lentiviral VaccinesДокумент10 страницGood Cop, Bad Cop? Interrogating The Immune Responses To Primate Lentiviral VaccinesMuhafizОценок пока нет
- Case 17 HIV-1Документ19 страницCase 17 HIV-1ngОценок пока нет
- Jem 194101395Документ12 страницJem 194101395Hamza WELGOОценок пока нет
- 140794.3 20210324105625 CoveredДокумент16 страниц140794.3 20210324105625 CoveredBruno RamírezОценок пока нет
- Towards An Epitope-Based Human Vaccine For Influenza: Tamar Ben-Yedidia Ruth ArnonДокумент7 страницTowards An Epitope-Based Human Vaccine For Influenza: Tamar Ben-Yedidia Ruth ArnonPCRMANОценок пока нет
- Therapy For Persistent HIVДокумент6 страницTherapy For Persistent HIVAnonymous ceYk4p4Оценок пока нет
- Human Papillomavirus Vaccine: History, Immunology, Current Status, and Future ProspectsДокумент15 страницHuman Papillomavirus Vaccine: History, Immunology, Current Status, and Future Prospectsnohora parradoОценок пока нет
- Hepatitis E Virus (HEV) - Specific T-Cell Responses Are Associated With Control of HEV InfectionДокумент14 страницHepatitis E Virus (HEV) - Specific T-Cell Responses Are Associated With Control of HEV Infectionchanchalv_678018469Оценок пока нет
- Working Paper 3 h5n1Документ7 страницWorking Paper 3 h5n1vijayОценок пока нет
- Editorial Overview Hildegund CJ Ertl and Antonio LanzavecchiaДокумент3 страницыEditorial Overview Hildegund CJ Ertl and Antonio Lanzavecchiahoangan118Оценок пока нет
- Ac and VaccineДокумент15 страницAc and VaccineMayaLunaОценок пока нет
- HIV Vaccine DevelopmentДокумент12 страницHIV Vaccine DevelopmentNarendra Kumar S.Оценок пока нет
- Weekly Epidemiological Report: A Publication of The Epidemiology Unit Ministry of HealthДокумент4 страницыWeekly Epidemiological Report: A Publication of The Epidemiology Unit Ministry of HealthNeranga Pravin SamaratungeОценок пока нет
- Mourtzoukou Et Al-2008-British Journal of SurgeryДокумент8 страницMourtzoukou Et Al-2008-British Journal of SurgeryTony AdeosunОценок пока нет
- montoya2007Документ2 страницыmontoya2007Monica Aleja FernándezОценок пока нет
- Immune Response To HIVДокумент9 страницImmune Response To HIVTugas HeinzОценок пока нет
- Novel COVID-19 Vaccine For Patients With Blood CancersДокумент3 страницыNovel COVID-19 Vaccine For Patients With Blood CancerslocosaltelefonoОценок пока нет
- Medical Progress: H C V IДокумент16 страницMedical Progress: H C V IriahОценок пока нет
- Immunizations in HIV PtsДокумент5 страницImmunizations in HIV PtsmhchristensenОценок пока нет
- Johnston 2007Документ9 страницJohnston 2007MedranoReyesLuisinОценок пока нет
- Shedding of Infectious Sars-Cov-2 Despite Vaccination When The Delta Variant Is Prevalent - Wisconsin, July 2021Документ9 страницShedding of Infectious Sars-Cov-2 Despite Vaccination When The Delta Variant Is Prevalent - Wisconsin, July 2021Micheal NicolucciОценок пока нет
- Post Covid ImmunityДокумент2 страницыPost Covid ImmunityIheb LouetiОценок пока нет
- Medical Progress: H C V IДокумент16 страницMedical Progress: H C V ITrisya Bella FibriantiОценок пока нет
- Correlates of Protection Against Symptomatic and Asymptomatic Sars-Cov-2 InfectionДокумент31 страницаCorrelates of Protection Against Symptomatic and Asymptomatic Sars-Cov-2 InfectionAbasyakira RaihanОценок пока нет
- VaccineДокумент7 страницVaccineRong LiuОценок пока нет
- Schiller JT - 09Документ6 страницSchiller JT - 09Bruno RalhaОценок пока нет
- gannavaram2014Документ10 страницgannavaram2014Shital BishtОценок пока нет
- Vassilopoulos 2002Документ13 страницVassilopoulos 2002deliaОценок пока нет
- Nihms 839861Документ40 страницNihms 839861Faisal JamshedОценок пока нет
- 141 Research Studies Affirm Naturally Acquired Immunity To Covid-19 (Brownstone Institute 2021)Документ40 страниц141 Research Studies Affirm Naturally Acquired Immunity To Covid-19 (Brownstone Institute 2021)gd_hbarОценок пока нет
- Paediatric AIDSДокумент52 страницыPaediatric AIDSvijayasree bavireddyОценок пока нет
- GetahunLTBINEJM2015 PDFДокумент9 страницGetahunLTBINEJM2015 PDFSharah Stephanie IIОценок пока нет
- IAS 2017: VRC01 Antibody Can Delay But Not Prevent HIV ReboundДокумент2 страницыIAS 2017: VRC01 Antibody Can Delay But Not Prevent HIV ReboundAriani AdeОценок пока нет
- Feb 2019Документ7 страницFeb 2019Siti AlfianaОценок пока нет
- Extra-Epitopic Hepatitis C Virus Polymorphisms Confer Resistance To Broadly Neutralizing Antibodies by Modulating Binding To Scavenger Receptor B1Документ25 страницExtra-Epitopic Hepatitis C Virus Polymorphisms Confer Resistance To Broadly Neutralizing Antibodies by Modulating Binding To Scavenger Receptor B1Albert Antonio Flores MejiaОценок пока нет
- Wolfram, 2013 PDFДокумент25 страницWolfram, 2013 PDFmangiemrОценок пока нет
- Patogenesis Del VIHДокумент19 страницPatogenesis Del VIHapi-3771611Оценок пока нет
- Artigo ImunologiaДокумент15 страницArtigo ImunologiaHugo RodriguesОценок пока нет
- 1 SMДокумент55 страниц1 SMCharlotteОценок пока нет
- Jurnal 1Документ9 страницJurnal 1Riyan TrequartistaОценок пока нет
- Hepatitis B and The Need For A Booster DoseДокумент8 страницHepatitis B and The Need For A Booster DoseMekar PalupiОценок пока нет
- Adenovirus Review - 2011Документ18 страницAdenovirus Review - 2011Julio Andrés Leiva ValdésОценок пока нет
- Khvi 17 1819742Документ24 страницыKhvi 17 1819742Sebastian BurgosОценок пока нет
- Management of Hepatitis C VirusДокумент15 страницManagement of Hepatitis C VirusahmedlakhaОценок пока нет
- Metapopulation ModellingДокумент25 страницMetapopulation Modellingjolamo1122916Оценок пока нет
- Nature 2020 AdeДокумент11 страницNature 2020 AdeGabrielaОценок пока нет
- Hepatitis Vaccines: Keywords: Hepatitis A, B, C, D, and E VaccinesДокумент18 страницHepatitis Vaccines: Keywords: Hepatitis A, B, C, D, and E VaccinesPutri Anita AchmadОценок пока нет
- (2, 2021) Thapsigargin and Respiratory VirusesДокумент19 страниц(2, 2021) Thapsigargin and Respiratory VirusesHannahОценок пока нет
- Tion at December 2021Документ10 страницTion at December 2021roquessudeОценок пока нет
- Lakshmanappa Et Al. - 2021 - SARS-CoV-2 Induces Robust Germinal Center CD4 T Follicular Helper Cell Responses in Rhesus Macaques - NaturДокумент14 страницLakshmanappa Et Al. - 2021 - SARS-CoV-2 Induces Robust Germinal Center CD4 T Follicular Helper Cell Responses in Rhesus Macaques - NaturCarlОценок пока нет
- Vaccination of Healthcare Workers A ReviewДокумент17 страницVaccination of Healthcare Workers A Reviewy2h996tnp8Оценок пока нет
- TUBE MostCited 1Документ6 страницTUBE MostCited 1jibin2008Оценок пока нет
- Models of Protection Against HIV/SIV: Models of Protection Against HIV/SIVОт EverandModels of Protection Against HIV/SIV: Models of Protection Against HIV/SIVGianfranco PancinoОценок пока нет
- Pathology-GIT Answered EssayДокумент33 страницыPathology-GIT Answered EssayRancesh FamoОценок пока нет
- Microbiology - VirologyДокумент34 страницыMicrobiology - VirologySasi DharanОценок пока нет
- Heroin in ColoradoДокумент62 страницыHeroin in ColoradoMichael_Lee_RobertsОценок пока нет
- Mathew-Majus EMQ BookДокумент210 страницMathew-Majus EMQ Booksessary1Оценок пока нет
- Viral PathogenesisДокумент8 страницViral PathogenesisBiofilm NSTUОценок пока нет
- New Microsoft Word DocumentДокумент4 страницыNew Microsoft Word DocumentMuhammad Sohail TariqОценок пока нет
- Wellens' Syndrome ECG Changes Predict Critical LAD StenosisДокумент79 страницWellens' Syndrome ECG Changes Predict Critical LAD Stenosiszehra khowajaОценок пока нет
- Manual ObsteДокумент1 237 страницManual ObsterobingpОценок пока нет
- Kode Icd 10Документ876 страницKode Icd 10Angga WarismanОценок пока нет
- Organ Function Test: Assessment of Functions of The OrgansДокумент39 страницOrgan Function Test: Assessment of Functions of The OrgansSri Abinash MishraОценок пока нет
- Noninvasive Assessment of Hepatic Fibrosis - Overview of Serologic Tests and Imaging Examinations - UpToDateДокумент35 страницNoninvasive Assessment of Hepatic Fibrosis - Overview of Serologic Tests and Imaging Examinations - UpToDatepopasorinemilianОценок пока нет
- Product Catalog 2020: New Poct SolutionДокумент20 страницProduct Catalog 2020: New Poct SolutionDave LuceroОценок пока нет
- Journal Club Hepatitis BДокумент45 страницJournal Club Hepatitis BMadeeha ArifОценок пока нет
- Clinical Practice Guidelines 11-18Документ20 страницClinical Practice Guidelines 11-18Feroz RaZa SoomrOoОценок пока нет
- Adazes WorkДокумент66 страницAdazes WorkAdemolaОценок пока нет
- Insert Hep B Engerix-BДокумент16 страницInsert Hep B Engerix-BshifanahmedОценок пока нет
- Pregnancy Risk AssessmentДокумент6 страницPregnancy Risk AssessmentSTEVEN DELAHUNTYОценок пока нет
- Hepatitis B in PregnancyДокумент6 страницHepatitis B in PregnancyherryОценок пока нет
- Lab Value MnemonicsДокумент10 страницLab Value MnemonicsSophia CuertoОценок пока нет
- Awareness On HepatitisДокумент52 страницыAwareness On HepatitisMizanur RahmanОценок пока нет
- Plasma ProteinsДокумент44 страницыPlasma ProteinsTinta Jisha AnaswaraОценок пока нет
- Viral Hepatitis in ChildrenДокумент15 страницViral Hepatitis in ChildrenDr AnilОценок пока нет
- HD Guideline Cleaning Disinfecting HD MachinesДокумент14 страницHD Guideline Cleaning Disinfecting HD MachinesMendes NovatoОценок пока нет
- Hepatitis A /BДокумент79 страницHepatitis A /BnasibdinОценок пока нет
- Hepatitis B Vaccination Waiver FormДокумент1 страницаHepatitis B Vaccination Waiver Formemmanuel espidaОценок пока нет
- Borang HirarcДокумент41 страницаBorang Hirarcnailul muna binti ahmad musadadОценок пока нет
- Final MBBS Part 1 Classes Schedule - Live UpdateДокумент6 страницFinal MBBS Part 1 Classes Schedule - Live UpdateKrishna VamsiОценок пока нет
- Cholestatic Hepatitis CaseДокумент3 страницыCholestatic Hepatitis CaseIndra YaniОценок пока нет
- Who Guidelines Blood Donor Selection 2012Документ126 страницWho Guidelines Blood Donor Selection 2012Dananjaya Junior100% (1)
- Clinical ExaminationsДокумент1 596 страницClinical ExaminationsmdasОценок пока нет