Вам также может понравиться
- DEFIBrilatorДокумент43 страницыDEFIBrilatoranon_632568468Оценок пока нет
- Emergency Medicine 1st Edition - DR - Waleed (101 Papers)Документ101 страницаEmergency Medicine 1st Edition - DR - Waleed (101 Papers)Mokhtar Moh100% (1)
- Cardiac ArrestДокумент14 страницCardiac ArrestCloudySkyОценок пока нет
- 2014 February ALS Cardiac Arrest and ROSCДокумент37 страниц2014 February ALS Cardiac Arrest and ROSCAuliaFadhilahTasruddinОценок пока нет
- Basic Life SupportДокумент6 страницBasic Life SupportArmin Tordecilla MercadoОценок пока нет
- Emmergency MedicineДокумент48 страницEmmergency MedicineSherein HagrasОценок пока нет
- Cardiac ArrestДокумент79 страницCardiac Arrestnaveena reddyОценок пока нет
- Stabilisasi Resp & HemidinamikДокумент30 страницStabilisasi Resp & HemidinamikBetrice KotanОценок пока нет
- Basic Life Support (BLS) and Advanced Cardiovascular Life Support (ACLS)Документ35 страницBasic Life Support (BLS) and Advanced Cardiovascular Life Support (ACLS)rajОценок пока нет
- 099 B SaroshДокумент14 страниц099 B SaroshUmair AnsariОценок пока нет
- Dvanced Cardiac Life SupportДокумент72 страницыDvanced Cardiac Life Supportolivia100% (1)
- DefibrillatorДокумент10 страницDefibrillatorMakhanVermaОценок пока нет
- BLS, ACLS DR Dagmawi FebrauruyДокумент33 страницыBLS, ACLS DR Dagmawi FebrauruyTemesgen GeletaОценок пока нет
- Cardiac ArrestДокумент30 страницCardiac ArrestagnescheruseryОценок пока нет
- CSS - Advanced Life SupportДокумент16 страницCSS - Advanced Life SupportnrahmaОценок пока нет
- Advanced Cardiac Life SupportДокумент28 страницAdvanced Cardiac Life SupportAbdulrahman AlsayyedОценок пока нет
- Pedia Advance-Cardiac-Life-SupportДокумент18 страницPedia Advance-Cardiac-Life-SupportTiffany AdriasОценок пока нет
- ACLS Handout As of 7-19-07Документ42 страницыACLS Handout As of 7-19-07Ganesh JadhavОценок пока нет
- Basic Life Support and Advanced Cardiovascular Life SupportДокумент90 страницBasic Life Support and Advanced Cardiovascular Life SupportRakhshanda khan100% (1)
- Advanced Cardiac Life Support: Valentina, MD, FIHAДокумент34 страницыAdvanced Cardiac Life Support: Valentina, MD, FIHAfaradibaОценок пока нет
- Advanced Cardiac Life SupportДокумент38 страницAdvanced Cardiac Life Supporthorosu100% (1)
- Life Threatening Arrhythmia and ManagementДокумент40 страницLife Threatening Arrhythmia and ManagementRuki HartawanОценок пока нет
- ACLS II Sept 25 StudentsДокумент60 страницACLS II Sept 25 StudentsLex CatОценок пока нет
- Bls (Basic Life Support) & Acls (Advanced Care Life Support) : PresenterДокумент135 страницBls (Basic Life Support) & Acls (Advanced Care Life Support) : PresenterbernarduswidodoОценок пока нет
- Bls (Basic Life Support) & Acls (Advanced Care Life Support) : PresenterДокумент135 страницBls (Basic Life Support) & Acls (Advanced Care Life Support) : PresenterbernarduswidodoОценок пока нет
- Unit 5 Cardiac Emergencies: StructureДокумент27 страницUnit 5 Cardiac Emergencies: StructurebtaleraОценок пока нет
- Cardiorespiratory ArrestДокумент51 страницаCardiorespiratory ArrestIrham KhairiОценок пока нет
- MylatestSOS BLS ACLS LectureДокумент87 страницMylatestSOS BLS ACLS LectureArmin MercadoОценок пока нет
- A (ACLS) - 2015: Dvanced Cardiac Life SupportДокумент52 страницыA (ACLS) - 2015: Dvanced Cardiac Life SupportNajmussaqibОценок пока нет
- Defibrillation and CardioversionДокумент51 страницаDefibrillation and CardioversionChinju Cyril100% (2)
- Minimalist Introduction To Anesthesiology Rev 1.5Документ12 страницMinimalist Introduction To Anesthesiology Rev 1.5Syafiqah HaniОценок пока нет
- Adult Advanced Life SupportДокумент23 страницыAdult Advanced Life SupportbigpriapОценок пока нет
- Acls Seminar MeДокумент62 страницыAcls Seminar MeAbnet Wondimu100% (1)
- ACLS PresentationДокумент79 страницACLS PresentationHumaira YasserОценок пока нет
- Immediate Life Support for healthcare Practitioners: A Step-By-Step GuideОт EverandImmediate Life Support for healthcare Practitioners: A Step-By-Step GuideОценок пока нет
- 3 Pulseless Arrest - Non-Shockable RhythmsДокумент29 страниц3 Pulseless Arrest - Non-Shockable RhythmsTejas Vivek WaghОценок пока нет
- BCLS 2Документ73 страницыBCLS 2Praveen Ravishankaran100% (1)
- Advanced Life Support (ALS)Документ4 страницыAdvanced Life Support (ALS)Lori BeckОценок пока нет
- ACLS Saroa Et AlДокумент17 страницACLS Saroa Et AlMarc Andreo MalalaОценок пока нет
- Cals ReviewbjvjvjДокумент14 страницCals ReviewbjvjvjCarl Jay M Ocariza100% (1)
- American Heart Association Guidelines For CPR 2015: Wanida Chongarunngamsang, MD. Faculty of Srinakarinwirot UniversityДокумент49 страницAmerican Heart Association Guidelines For CPR 2015: Wanida Chongarunngamsang, MD. Faculty of Srinakarinwirot UniversityZulkarnainBustamamОценок пока нет
- Cardiorespiratory Arrest (FS)Документ88 страницCardiorespiratory Arrest (FS)haerul ikhsanОценок пока нет
- Code Blue Procedures: Luis Enriquez RN, BSДокумент25 страницCode Blue Procedures: Luis Enriquez RN, BSsyahputra88Оценок пока нет
- Medip, IJAM-724 CДокумент3 страницыMedip, IJAM-724 CKhalilSemlaliОценок пока нет
- Advanced Cardiac Life Support Information From American Heart Association, Advanced Cardiac Life Support, 2006Документ25 страницAdvanced Cardiac Life Support Information From American Heart Association, Advanced Cardiac Life Support, 2006karento1Оценок пока нет
- Er Rotation - Ecg & BlsДокумент39 страницEr Rotation - Ecg & BlsJEDIDIAH ALOMBROОценок пока нет
- CPCRДокумент51 страницаCPCRAnushaОценок пока нет
- Anaesthetic Crisis ManualДокумент63 страницыAnaesthetic Crisis ManualkushishaОценок пока нет
- Incorrect - Right Answer: True: CorrectДокумент10 страницIncorrect - Right Answer: True: CorrectAhmed - Sawalha100% (2)
- Bls & Acls & DC ShockДокумент70 страницBls & Acls & DC Shockpop lopОценок пока нет
- Chapter3Shock CirculationДокумент13 страницChapter3Shock CirculationSri AgustinaОценок пока нет
- Advanced Cardiac Life Support (ACLS) : By: Diana Blum MSN Metropolitan Community College Nursing 2150Документ16 страницAdvanced Cardiac Life Support (ACLS) : By: Diana Blum MSN Metropolitan Community College Nursing 2150Vikneswara SoorianarayananОценок пока нет
- Chain of SurvivalДокумент4 страницыChain of Survivalgurneet kourОценок пока нет
- Departemen Kardiologi FK USU RSUP. H. Adam Malik MedanДокумент64 страницыDepartemen Kardiologi FK USU RSUP. H. Adam Malik MedanBonitavanyОценок пока нет
- Code Blue (Autosaved)Документ24 страницыCode Blue (Autosaved)irfan taibОценок пока нет
- Medical and Surgical Nursing: Cardiopulmonary ResuscitationДокумент54 страницыMedical and Surgical Nursing: Cardiopulmonary ResuscitationRiteka SinghОценок пока нет
- Questions and Answers in Small Animal AnesthesiaОт EverandQuestions and Answers in Small Animal AnesthesiaLesley J. SmithОценок пока нет
- Advanced Neonatal Procedures2Документ14 страницAdvanced Neonatal Procedures2Vijith.V.kumar100% (8)
- Occipito Posterior PositionДокумент52 страницыOccipito Posterior PositionVijith.V.kumar100% (3)
- Breast CancerДокумент15 страницBreast CancerVijith.V.kumar100% (2)
- CPDДокумент45 страницCPDVijith.V.kumar100% (1)
- Forceps DeliveryДокумент32 страницыForceps DeliveryVijith.V.kumar50% (2)
- Expanded RoleДокумент19 страницExpanded RoleVijith.V.kumar100% (2)
- Premature BabyДокумент41 страницаPremature BabyVijith.V.kumar100% (9)
- Gynecological DisordersДокумент26 страницGynecological DisordersVijith.V.kumarОценок пока нет
- Uterine Anomaly, Fibroid Uterus, Ovarian Tumor, Uterine ProlapseДокумент30 страницUterine Anomaly, Fibroid Uterus, Ovarian Tumor, Uterine ProlapseVijith.V.kumar80% (5)
- Breech PresentationДокумент53 страницыBreech PresentationVijith.V.kumar100% (6)
- Records and ReportsДокумент6 страницRecords and ReportsVijith.V.kumar100% (5)
- Staff Orientation, Training and DevelopmentДокумент57 страницStaff Orientation, Training and DevelopmentVijith.V.kumarОценок пока нет
- Intranatal Assessment Kempegowda College of Nursing, V.V.Puram, B'Lore-04Документ8 страницIntranatal Assessment Kempegowda College of Nursing, V.V.Puram, B'Lore-04Vijith.V.kumar100% (1)
- Kempegowda College of Nursing: Subject: Obstetric and Gynaecological NursingДокумент2 страницыKempegowda College of Nursing: Subject: Obstetric and Gynaecological NursingVijith.V.kumarОценок пока нет
- Neonatal NursingДокумент2 страницыNeonatal NursingVijith.V.kumarОценок пока нет
- Diet During PregnancyДокумент14 страницDiet During PregnancyVijith.V.kumarОценок пока нет
- High Risk NewbornДокумент76 страницHigh Risk NewbornVijith.V.kumar91% (22)
- Obstetric EmergenciesДокумент44 страницыObstetric EmergenciesVijith.V.kumarОценок пока нет
- Destructive Operation and Caesarian SectionДокумент53 страницыDestructive Operation and Caesarian SectionVijith.V.kumar0% (1)
- Phisiological Changes Due To PregnancyДокумент21 страницаPhisiological Changes Due To PregnancyVijith.V.kumarОценок пока нет
- Antenatal PreparationДокумент47 страницAntenatal PreparationVijith.V.kumarОценок пока нет
- Analgesia and Anesthesia in ObstetricsДокумент8 страницAnalgesia and Anesthesia in ObstetricsVijith.V.kumar100% (3)
- OccipitoposteriorДокумент11 страницOccipitoposteriorVijith.V.kumar100% (1)
- EngorgementДокумент1 страницаEngorgementVijith.V.kumarОценок пока нет
- Inservice EducationДокумент4 страницыInservice EducationVijith.V.kumar50% (2)
- Staff Orientation, Training and DevelopmentДокумент57 страницStaff Orientation, Training and DevelopmentVijith.V.kumarОценок пока нет
- Antenatal Assessment FormatДокумент9 страницAntenatal Assessment FormatVijith.V.kumar93% (14)
- Depression - 9 Nursing Diagnosis Care PlanДокумент2 страницыDepression - 9 Nursing Diagnosis Care PlanVijith.V.kumarОценок пока нет
- Anecdotal RecordДокумент13 страницAnecdotal RecordVijith.V.kumar100% (1)
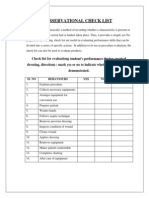
- 30.observational Check ListДокумент1 страница30.observational Check ListVijith.V.kumarОценок пока нет
- Pharmacology MCQs 2Документ6 страницPharmacology MCQs 2Waseem SarwarОценок пока нет
- AntihistamineДокумент16 страницAntihistamine30068Оценок пока нет
- General PharmacologyДокумент32 страницыGeneral PharmacologyAlphahin 17Оценок пока нет
- Details of Conscious Caring: Product CatalogueДокумент6 страницDetails of Conscious Caring: Product CatalogueBaharОценок пока нет
- Blood Components Dosage and Their Administration (Compatibility Mode)Документ7 страницBlood Components Dosage and Their Administration (Compatibility Mode)Chandra SekarОценок пока нет
- Jurnal Hukum Dan Etika Kesehatan: Penggunaan Ganja Medis Dalam Pengobatan Rasional Dan Pengaturannya Di IndonesiaДокумент13 страницJurnal Hukum Dan Etika Kesehatan: Penggunaan Ganja Medis Dalam Pengobatan Rasional Dan Pengaturannya Di IndonesiaWidia MuniraОценок пока нет
- DS PNSSДокумент4 страницыDS PNSSKathryne May JinonОценок пока нет
- Role of Chemotherapy in Malignant Ovarian TumorsДокумент36 страницRole of Chemotherapy in Malignant Ovarian TumorsUsha AnengaОценок пока нет
- Pulseless Arrest Algorithm For Managing VF and Pulseless VTДокумент3 страницыPulseless Arrest Algorithm For Managing VF and Pulseless VTLaili CinthiaОценок пока нет
- Drugs and DosagesДокумент4 страницыDrugs and DosagesDin-Din Que33% (3)
- Philippine LawsДокумент1 страницаPhilippine LawsWenn Joyrenz ManeclangОценок пока нет
- Gambro Phoenix SystemДокумент2 страницыGambro Phoenix SystemGraham Thomas GipsonОценок пока нет
- Kubie, L. (1971) - The Destructive Potential of Humor in PsychotherapyДокумент6 страницKubie, L. (1971) - The Destructive Potential of Humor in PsychotherapyMikaelaMundell100% (1)
- NARCOTIC&CONTROLLEDДокумент56 страницNARCOTIC&CONTROLLEDMelai Rodriguez IbardalozaОценок пока нет
- Thymus Vulgaris - TimijanДокумент8 страницThymus Vulgaris - TimijanRok KopinčОценок пока нет
- Check List First AidДокумент6 страницCheck List First AidNatasha VanyaОценок пока нет
- CLINICAL MENTORING 21 TERAPI CAIRAN PADA KASUS GAWAT DARURAT OLEH Dr. HADIKI HABIB SP - PD - PDFДокумент21 страницаCLINICAL MENTORING 21 TERAPI CAIRAN PADA KASUS GAWAT DARURAT OLEH Dr. HADIKI HABIB SP - PD - PDFwindyani hardiОценок пока нет
- NOEL and MACO Calculations in Cleaning Validation - Pharmaceutical GuidelinesДокумент1 страницаNOEL and MACO Calculations in Cleaning Validation - Pharmaceutical GuidelinesDrSunil gvalaniОценок пока нет
- BupropionДокумент23 страницыBupropiontheintrovОценок пока нет
- Telmisartan Amlodipine Single Pill Combination In.6Документ12 страницTelmisartan Amlodipine Single Pill Combination In.6urbanincultureОценок пока нет
- WHO MDR 2020 Handbook Treatment PDFДокумент88 страницWHO MDR 2020 Handbook Treatment PDFYuanita GunawanОценок пока нет
- Glyburide (Glibenclamide) : Drug Information: Brand Names: USДокумент17 страницGlyburide (Glibenclamide) : Drug Information: Brand Names: USAnonymous wmF9p2ejОценок пока нет
- Drug Senna Drug CardДокумент1 страницаDrug Senna Drug CardSrkocher100% (2)
- Drug Management Cycle: Adryan Fristiohady Program Studi Pendidikan Profesi Apoteker Universitas Halu OleoДокумент34 страницыDrug Management Cycle: Adryan Fristiohady Program Studi Pendidikan Profesi Apoteker Universitas Halu OleoLhynda Priarti Latif100% (4)
- Medication: Expected Pharmacological Action Therapeutic UseДокумент1 страницаMedication: Expected Pharmacological Action Therapeutic UseAli GarciaОценок пока нет
- Hi Alert MedicationsHHHIGHДокумент27 страницHi Alert MedicationsHHHIGHnovitalumintusariОценок пока нет
- 70661-483430ZIMPEL 2020 Terapias Complementares e Alternativas para o Alavio Da Dor PasacesarianaДокумент147 страниц70661-483430ZIMPEL 2020 Terapias Complementares e Alternativas para o Alavio Da Dor PasacesarianaDanúbia OliveiraОценок пока нет
- Drug Study TheophyllineДокумент1 страницаDrug Study Theophyllinevaldez.adler.lОценок пока нет
- Daftar Obat IGD Dan Poli UmumДокумент2 страницыDaftar Obat IGD Dan Poli UmumPku Aisyiyah JeparaОценок пока нет
- 2022 American Society of Anesthesiologists Practice GuidelinesДокумент7 страниц2022 American Society of Anesthesiologists Practice GuidelinesIrving Alexis Pérez DuqueОценок пока нет