Вам также может понравиться
- Commercial Dispatch Eedition 6-13-19Документ12 страницCommercial Dispatch Eedition 6-13-19The Dispatch100% (1)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Grid / Hippodamian Model: Hippodamus of MiletusДокумент34 страницыGrid / Hippodamian Model: Hippodamus of MiletusVriti SachdevaОценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5795)
- đề thi TAДокумент15 страницđề thi TAĐào Nguyễn Duy TùngОценок пока нет
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Ernieta - Entrep Survey Act.Документ6 страницErnieta - Entrep Survey Act.Nichole John ErnietaОценок пока нет
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- FINAL Parent Handbook AitchisonДокумент68 страницFINAL Parent Handbook AitchisonSaeed AhmedОценок пока нет
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- Tolkien Essay-TreesДокумент10 страницTolkien Essay-Treesapi-657753727Оценок пока нет
- Cu 5 - The Law Enforcement Pillar Part 2Документ22 страницыCu 5 - The Law Enforcement Pillar Part 2marygrace.sacbibit.lawОценок пока нет
- Effects of Changes in Foreign Exchange Rates Ias 21Документ11 страницEffects of Changes in Foreign Exchange Rates Ias 21cykenОценок пока нет
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Basketball Coaching ToolboxДокумент71 страницаBasketball Coaching Toolboxmensrea0Оценок пока нет
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Easy Trade Manager Forex RobotДокумент10 страницEasy Trade Manager Forex RobotPinda DhanoyaОценок пока нет
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Solution ManualДокумент40 страницSolution Manualkhaled_behery9934100% (1)
- West Visayas State University (CHECKLIST FOR FS)Документ3 страницыWest Visayas State University (CHECKLIST FOR FS)Nichole Manalo - PoticarОценок пока нет
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Time Value of Money PDFДокумент4 страницыTime Value of Money PDFCalvin SandiОценок пока нет
- Coin Operated Short Movie AnalysisДокумент17 страницCoin Operated Short Movie AnalysisA 29 Nathaniela Devany MiramaОценок пока нет
- Pineapple Working PaperДокумент57 страницPineapple Working PaperAnonymous EAineTiz100% (7)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Exploration of MoonДокумент8 страницExploration of MoonAryan KhannaОценок пока нет
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
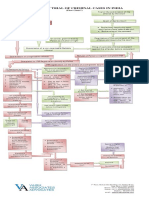
- Process of Trial of Criminal Cases in India (Flow Chart)Документ1 страницаProcess of Trial of Criminal Cases in India (Flow Chart)Arun Hiro100% (1)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Untitled PresentationДокумент23 страницыUntitled Presentationapi-543394268Оценок пока нет
- Jurnal Inggris CyberДокумент7 страницJurnal Inggris Cybertamara amandaОценок пока нет
- CJ1W-PRT21 PROFIBUS-DP Slave Unit: Operation ManualДокумент100 страницCJ1W-PRT21 PROFIBUS-DP Slave Unit: Operation ManualSergio Eu CaОценок пока нет
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Alternating Voltage and CurrentДокумент41 страницаAlternating Voltage and CurrentKARTHIK LОценок пока нет
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1091)
- Leaders Eat Last Key PointsДокумент8 страницLeaders Eat Last Key Pointsfidoja100% (2)
- Igice Cya Kabiri: 2.0. Intambwe Zitandukanye Z'Imikorere Ya Mariyamu KinyamaruraДокумент7 страницIgice Cya Kabiri: 2.0. Intambwe Zitandukanye Z'Imikorere Ya Mariyamu KinyamaruraJacques Abimanikunda BarahirwaОценок пока нет
- AIPT 2021 GuidelineДокумент4 страницыAIPT 2021 GuidelineThsavi WijayasingheОценок пока нет
- Grimshaw v. Ford Motor CoДокумент35 страницGrimshaw v. Ford Motor CozichenОценок пока нет
- Programming Essentials in PythonДокумент23 страницыProgramming Essentials in PythonNabeel AmjadОценок пока нет
- Sara Lee: A Tale of Another Turnaround: Case Analysis - Strategic ManagementДокумент6 страницSara Lee: A Tale of Another Turnaround: Case Analysis - Strategic ManagementKeerthi PurushothamanОценок пока нет
- Righeimer ComplaintДокумент45 страницRigheimer ComplaintSarah BatchaОценок пока нет
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- John Lear UFO Coverup RevelationsДокумент30 страницJohn Lear UFO Coverup RevelationscorneliusgummerichОценок пока нет
- ShowBoats International (May 2016)Документ186 страницShowBoats International (May 2016)LelosPinelos123100% (1)