Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Nolei Belarmino CVДокумент2 страницыNolei Belarmino CVti noleiОценок пока нет
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- LL Dece Standards Fulldraft9Документ370 страницLL Dece Standards Fulldraft9api-523534173Оценок пока нет
- Observation Sheet FsДокумент2 страницыObservation Sheet FsDolly ManaloОценок пока нет
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- JH JW Leveled Lesson PlanДокумент3 страницыJH JW Leveled Lesson Planapi-314361473Оценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- EMasters Student HandbookДокумент48 страницEMasters Student Handbookharikevadiya4Оценок пока нет
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Capstone Project ModuleДокумент12 страницCapstone Project ModuleJeffrey MasicapОценок пока нет
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Day 1Документ16 страницDay 1Rehan HabibОценок пока нет
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- GR 5 Term 4 2017 Maths TrackerДокумент108 страницGR 5 Term 4 2017 Maths TrackerIrfaanОценок пока нет
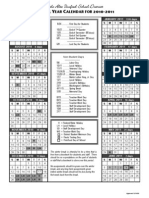
- PAUSD SchoolYearCalendar2010Документ1 страницаPAUSD SchoolYearCalendar2010Justin HolmgrenОценок пока нет
- 10 đề ôn luyện Tiếng Anh học kì I lớp 12Документ46 страниц10 đề ôn luyện Tiếng Anh học kì I lớp 12NguyenNgocОценок пока нет
- B Tech Results - CompressedДокумент2 страницыB Tech Results - CompressedRajnikant YadavОценок пока нет
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Barclays Life Skills (F2F) JOB READINESS WORKSHOPДокумент2 страницыBarclays Life Skills (F2F) JOB READINESS WORKSHOPviraaj mehraОценок пока нет
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- 5e Lesson PlanДокумент4 страницы5e Lesson Planapi-354775391Оценок пока нет
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Assessment/ Checking of Outputs: H7GD-Ib-13Документ1 страницаAssessment/ Checking of Outputs: H7GD-Ib-13Raymund MativoОценок пока нет
- 39th IATLIS National Conference 2023Документ3 страницы39th IATLIS National Conference 2023Sukhdev SinghОценок пока нет
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Allied School System Internship ReportДокумент64 страницыAllied School System Internship Reportbbaahmad8963% (30)
- Standard Six Reading Program RationaleДокумент1 страницаStandard Six Reading Program Rationaleapi-278580587Оценок пока нет
- What Makes Continuing Education Effective PerspectДокумент6 страницWhat Makes Continuing Education Effective PerspecttestОценок пока нет
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Postgraduate - 17 January 2023Документ2 страницыPostgraduate - 17 January 2023Times MediaОценок пока нет
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Maths XiДокумент2 страницыMaths Xizy6136Оценок пока нет
- Special Education: Masters & Licensure ProgramsДокумент12 страницSpecial Education: Masters & Licensure Programsmgentry1Оценок пока нет
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- For University Stuttgart: Copies of QualificationsДокумент2 страницыFor University Stuttgart: Copies of QualificationsMJ GaleanoОценок пока нет
- Traditional vs. Online EducationДокумент5 страницTraditional vs. Online EducationEdilbert Bonifacio GayoОценок пока нет
- FRIT 7234 Ethical Use of Information Embedded LessonДокумент9 страницFRIT 7234 Ethical Use of Information Embedded LessonMunoОценок пока нет
- Senses Lesson PlanДокумент3 страницыSenses Lesson Planapi-134634747Оценок пока нет
- CNF DLL Week 5 q2Документ5 страницCNF DLL Week 5 q2Bethel MedalleОценок пока нет
- Don Marcos Rosales Elementary School Ipcrf-Development Plan: Department of EducationДокумент2 страницыDon Marcos Rosales Elementary School Ipcrf-Development Plan: Department of Educationmarilene figaresОценок пока нет
- Scholarship and Trainings For Filipino TeachersДокумент26 страницScholarship and Trainings For Filipino Teacherschoi_salazarОценок пока нет
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Sri Kumaran Children's Home - NurseryДокумент2 страницыSri Kumaran Children's Home - NurseryKrishna PrasadОценок пока нет
- Adapted From Ginger Tucker's First Year Teacher NotebookДокумент3 страницыAdapted From Ginger Tucker's First Year Teacher Notebookapi-349880083Оценок пока нет