Вам также может понравиться
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Myco Viro Notes Module 6Документ6 страницMyco Viro Notes Module 6Kyle Jude Roberts SanesОценок пока нет
- Mortality Report April 25th 2019Документ12 страницMortality Report April 25th 2019ramotОценок пока нет
- Udder & TeatДокумент23 страницыUdder & TeatAdarshBijapurОценок пока нет
- Drug Study Amlodipine & HydrocortisoneДокумент4 страницыDrug Study Amlodipine & HydrocortisoneJohn Kristoffer JisonОценок пока нет
- Annex 1 RSWITCH - Informed Consent - Forms - EnglishДокумент6 страницAnnex 1 RSWITCH - Informed Consent - Forms - Englishmerealemketema1Оценок пока нет
- KONSULTA 073123 v1Документ124 страницыKONSULTA 073123 v1Substationsix MalaboncpsОценок пока нет
- Diagnostic Tests PDFДокумент2 страницыDiagnostic Tests PDFBenedict AlvarezОценок пока нет
- ResumeДокумент5 страницResumeJuvie Dawn MaquilanОценок пока нет
- 1 s2.0 S0883540320304605 MainДокумент4 страницы1 s2.0 S0883540320304605 MainSavОценок пока нет
- Section Editor: Steven A. Newman, MD: J Neuro-Ophthalmol, Vol. 28, No. 4, 2008Документ10 страницSection Editor: Steven A. Newman, MD: J Neuro-Ophthalmol, Vol. 28, No. 4, 2008Jessica Leika MatibagОценок пока нет
- Module 6.2 - 2022Документ36 страницModule 6.2 - 2022Bogdan Roxana-MariaОценок пока нет
- SOP TEC 15 Calculating Drug Doses v1.1Документ2 страницыSOP TEC 15 Calculating Drug Doses v1.1rajenderizeОценок пока нет
- Pulmonary RehabilitationДокумент86 страницPulmonary RehabilitationJuanitoCabatañaLimIIIОценок пока нет
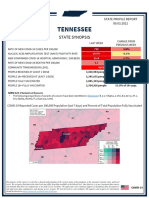
- Tennessee State Profile Report 20210903 PublicДокумент17 страницTennessee State Profile Report 20210903 PublicAnonymous GF8PPILW5Оценок пока нет
- Broad Spectrum AntibioticsДокумент17 страницBroad Spectrum AntibioticsRabi ShahОценок пока нет
- Effects of Timing of Appendectomy On The Risks of Perforation and Postoperative Complications of Acute AppendicitisДокумент9 страницEffects of Timing of Appendectomy On The Risks of Perforation and Postoperative Complications of Acute AppendicitisLydia EniithОценок пока нет
- Holy BasilДокумент1 страницаHoly BasilRichard SmithОценок пока нет
- Asfiksia JurnalДокумент9 страницAsfiksia JurnalGung Citra PratikaОценок пока нет
- OB Med 2023 FinalДокумент98 страницOB Med 2023 FinalBelinda ELISHAОценок пока нет
- Pharmacology For Nurses: A Pathophysiologic Approach: Fifth EditionДокумент31 страницаPharmacology For Nurses: A Pathophysiologic Approach: Fifth Editionadni_wgОценок пока нет
- 5 Drugs 1 IVДокумент10 страниц5 Drugs 1 IVBianca Nicole Gacad FernandezОценок пока нет
- Thalassemia: by M.Moazzam Siddiqui FA16-CVE-073Документ10 страницThalassemia: by M.Moazzam Siddiqui FA16-CVE-073Moazzam SiddiquiОценок пока нет
- SpecialistДокумент1 страницаSpecialistShashiОценок пока нет
- Gotthard Bulau Closed Water-Seal Drainage For Empyema,: John A. MeyerДокумент3 страницыGotthard Bulau Closed Water-Seal Drainage For Empyema,: John A. Meyerputri aprilianiОценок пока нет
- HTTP Healthmedicinet Com II 2013 8 PDFДокумент240 страницHTTP Healthmedicinet Com II 2013 8 PDFtuni santeОценок пока нет
- Shortage of Medication ArgumentДокумент5 страницShortage of Medication Argumentapi-543490444Оценок пока нет
- 0312 Antibody IdДокумент18 страниц0312 Antibody IdKen WayОценок пока нет
- Primay Health CentresДокумент100 страницPrimay Health CentresBirupakshya RoutОценок пока нет
- M104 - ExamДокумент8 страницM104 - ExamChrystal Anne Flores CorderoОценок пока нет
- Oral Comm - W4 - Answer SheetДокумент3 страницыOral Comm - W4 - Answer SheetKrista. meters100% (1)