Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Datasheet s5933Документ18 страницDatasheet s5933BuelnitaОценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- CR Mm3.0 Mammo CassetteДокумент2 страницыCR Mm3.0 Mammo CassetteBuelnitaОценок пока нет
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- PhilipsДокумент55 страницPhilipsSindy MtmОценок пока нет
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Introduction To X-Ray Equipment OperationДокумент43 страницыIntroduction To X-Ray Equipment OperationBuelnitaОценок пока нет
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Dental Equip 03Документ6 страницDental Equip 03BuelnitaОценок пока нет
- Introduction To X-Ray Equipment OperationДокумент43 страницыIntroduction To X-Ray Equipment OperationBuelnitaОценок пока нет
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- ISCD HologicImagingJankowskiДокумент22 страницыISCD HologicImagingJankowskiBuelnitaОценок пока нет
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- AN521 Intoduction To IGBTДокумент10 страницAN521 Intoduction To IGBTBuelnitaОценок пока нет
- Evol Ins and User ManДокумент113 страницEvol Ins and User Mancrischio52Оценок пока нет
- Short Form Specification: November 1, 1995Документ6 страницShort Form Specification: November 1, 1995BuelnitaОценок пока нет
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Flexowell® Replacement-Belts enДокумент3 страницыFlexowell® Replacement-Belts enrererererererererereОценок пока нет
- 2CCC413001C0203 S800Документ60 страниц2CCC413001C0203 S800Sang SekОценок пока нет
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Parker - Twin FilterДокумент6 страницParker - Twin FilterNAHASALI11Оценок пока нет
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Cbse Class 6 Science Notes Chapter 13Документ4 страницыCbse Class 6 Science Notes Chapter 13rohinimr007Оценок пока нет
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
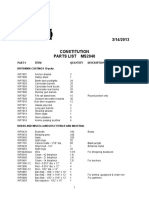
- MS2040 Constitution Parts ListДокумент6 страницMS2040 Constitution Parts ListTemptationОценок пока нет
- Pathoftherosesyllabus2015 1 PDFДокумент12 страницPathoftherosesyllabus2015 1 PDFsperm100% (7)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Aspen Tutorial #4: Design Specs & Sensitivity Analysis: OutlineДокумент11 страницAspen Tutorial #4: Design Specs & Sensitivity Analysis: OutlineWonda 005Оценок пока нет
- Looking For Cochlear Dead Regions A Clinical Experience With TEN TestДокумент9 страницLooking For Cochlear Dead Regions A Clinical Experience With TEN TestVinay S NОценок пока нет
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Manual CaladoraДокумент32 страницыManual CaladoraMiguel Angel Vega TrejoОценок пока нет
- IMDB - ColaboratoryДокумент10 страницIMDB - Colaboratory4416 LikhithaОценок пока нет
- Unit 21Документ22 страницыUnit 21Yuni IndahОценок пока нет
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Grade 6 2nd Periodical Test With TOS Answer Keys MATH 1 PDFДокумент6 страницGrade 6 2nd Periodical Test With TOS Answer Keys MATH 1 PDFmafeh caranogОценок пока нет
- Taiwan API Manufacturer ListДокумент4 страницыTaiwan API Manufacturer Listkalyani dynamicsОценок пока нет
- Philippine Airlines Reservation New Timings Dep - 230314 - 193643Документ7 страницPhilippine Airlines Reservation New Timings Dep - 230314 - 193643sophia buiserОценок пока нет
- N100 Rle Back MassageДокумент24 страницыN100 Rle Back MassagerlinaoОценок пока нет
- Y-7 Yoke: AC/DC Electromagnetic YokeДокумент2 страницыY-7 Yoke: AC/DC Electromagnetic YokeImmanuel RajОценок пока нет
- Buk Uuuuuu UuuuuuuДокумент92 страницыBuk Uuuuuu UuuuuuuJanaliyaОценок пока нет
- Author Name Title Paper/Submission ID Submission Date Total Pages Document TypeДокумент32 страницыAuthor Name Title Paper/Submission ID Submission Date Total Pages Document TypeArka ChakrabortyОценок пока нет
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Essentials of o Ste 00 DaveДокумент112 страницEssentials of o Ste 00 DaveGeki Iovan100% (1)
- kAmAxI Muka Panchashati EngДокумент25 страницkAmAxI Muka Panchashati EngSrinathvr100% (1)
- DinmjgДокумент10 страницDinmjghaker linkisОценок пока нет
- CP Lithium Ion BatteriesДокумент4 страницыCP Lithium Ion BatteriesvaseemalikhanОценок пока нет
- Power and Propulsion PDFДокумент13 страницPower and Propulsion PDFahmedalgaloОценок пока нет
- Form 03B Heritage Bell 1Документ2 страницыForm 03B Heritage Bell 1ValОценок пока нет
- ELK-3 550 1HC0000742AFEnДокумент20 страницELK-3 550 1HC0000742AFEnOnur FişekОценок пока нет
- TP260SR Tier 3 TC002-1037Документ1 страницаTP260SR Tier 3 TC002-1037Jorge GalarceОценок пока нет
- Las Mapeh 9 q2 w6 HealthДокумент8 страницLas Mapeh 9 q2 w6 HealthJemalyn Hibaya Lasaca100% (1)
- LEM 91-161 Fla E 0612Документ13 страницLEM 91-161 Fla E 0612Julen IturriozОценок пока нет
- Optimizing With eGaN FETsДокумент6 страницOptimizing With eGaN FETskhsniperОценок пока нет
- Hinomoto Tractor Parts Catalogue 2018 C144, C174, E150, E180, E230, E250, E280, E384Документ63 страницыHinomoto Tractor Parts Catalogue 2018 C144, C174, E150, E180, E230, E250, E280, E384Monica Mascarenhas0% (1)