Вам также может понравиться
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- 6th Central Pay Commission Salary CalculatorДокумент15 страниц6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- 6th Central Pay Commission Salary CalculatorДокумент15 страниц6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Poa SbaДокумент34 страницыPoa Sbaannmarie100% (2)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- PPT For Corporate ActionsДокумент29 страницPPT For Corporate Actionshimanshu9899Оценок пока нет
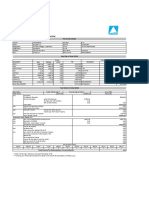
- Altruist Customer Management India PVT LTD: Personal DetailsДокумент1 страницаAltruist Customer Management India PVT LTD: Personal DetailsSampathKPОценок пока нет
- IFRS Adoption and Implementation in Korea, and The Lessons LearnedДокумент109 страницIFRS Adoption and Implementation in Korea, and The Lessons LearnedSu Li WenОценок пока нет
- Acquisition IntegrationДокумент24 страницыAcquisition IntegrationKannanОценок пока нет
- Pay For Performance and Financial Incentives: Gary DesslerДокумент35 страницPay For Performance and Financial Incentives: Gary DesslerNaeem KhanОценок пока нет
- CIR V PaДокумент9 страницCIR V PacrixzamОценок пока нет
- Department of Labor: Generalprovision 6 28 07Документ6 страницDepartment of Labor: Generalprovision 6 28 07USA_DepartmentOfLaborОценок пока нет
- Department of Labor: Aces CPДокумент36 страницDepartment of Labor: Aces CPUSA_DepartmentOfLabor100% (2)
- Department of Labor: YouthworkerДокумент1 страницаDepartment of Labor: YouthworkerUSA_DepartmentOfLaborОценок пока нет
- Department of Labor: Yr English GuideДокумент1 страницаDepartment of Labor: Yr English GuideUSA_DepartmentOfLaborОценок пока нет
- Department of Labor: YouthRulesBrochureДокумент12 страницDepartment of Labor: YouthRulesBrochureUSA_DepartmentOfLaborОценок пока нет
- Department of Labor: 20040422 YouthrulesДокумент1 страницаDepartment of Labor: 20040422 YouthrulesUSA_DepartmentOfLaborОценок пока нет
- Department of Labor: Niosh Recs To Dol 050302Документ198 страницDepartment of Labor: Niosh Recs To Dol 050302USA_DepartmentOfLaborОценок пока нет
- Department of Labor: ln61003Документ2 страницыDepartment of Labor: ln61003USA_DepartmentOfLaborОценок пока нет
- Department of Labor: Niosh Letter FinalДокумент3 страницыDepartment of Labor: Niosh Letter FinalUSA_DepartmentOfLaborОценок пока нет
- Department of Labor: JYMP 11x17 3Документ1 страницаDepartment of Labor: JYMP 11x17 3USA_DepartmentOfLaborОценок пока нет
- Department of Labor: Final ReportДокумент37 страницDepartment of Labor: Final ReportUSA_DepartmentOfLaborОценок пока нет
- Department of Labor: Yr English GuideДокумент1 страницаDepartment of Labor: Yr English GuideUSA_DepartmentOfLaborОценок пока нет
- College Savings Plan ComparisonДокумент2 страницыCollege Savings Plan Comparisoncharanmann9165Оценок пока нет
- List of Important Questions With Answers For Nov 2022 (R)Документ108 страницList of Important Questions With Answers For Nov 2022 (R)manuacreddyОценок пока нет
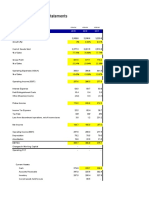
- Financial Statements-Kingsley AkinolaДокумент4 страницыFinancial Statements-Kingsley AkinolaKingsley AkinolaОценок пока нет
- Examples TransferpricingДокумент15 страницExamples Transferpricingpam7779Оценок пока нет
- Bacayo 07 Activity 1 EntrepДокумент3 страницыBacayo 07 Activity 1 EntrepDavid GutierrezОценок пока нет
- Sultan Mahmud: Road To BB Ad 2020Документ4 страницыSultan Mahmud: Road To BB Ad 2020TAWHIDОценок пока нет
- Accounting II FinalДокумент6 страницAccounting II FinalPak KhОценок пока нет
- McdonaldsДокумент77 страницMcdonaldsaster5262100% (1)
- Madras Labour UnionДокумент4 страницыMadras Labour UnionPraneeth ProdduturuОценок пока нет
- Chapter 12 Dividend Theory RelevancyДокумент38 страницChapter 12 Dividend Theory RelevancyAmir ArifОценок пока нет
- Dunkin Donuts - S1Документ410 страницDunkin Donuts - S1alex_winter_1Оценок пока нет
- An Introduction To Cost Terms and Purposes Homework 2-42, 46 2-42 Income Statement and Schedule of Cost of Goods Manufactured. Chan's ManufacturingДокумент3 страницыAn Introduction To Cost Terms and Purposes Homework 2-42, 46 2-42 Income Statement and Schedule of Cost of Goods Manufactured. Chan's ManufacturingCheuk Wai YEUNGОценок пока нет
- PowerPoint Slides PPEДокумент21 страницаPowerPoint Slides PPEAndrew ChongОценок пока нет
- GP 10 Table ReferenceДокумент569 страницGP 10 Table ReferencekempecОценок пока нет
- Letter To Bank For Interest Certi Cate of Fixed Deposit (FD) SampleДокумент6 страницLetter To Bank For Interest Certi Cate of Fixed Deposit (FD) SampleHackerzillaОценок пока нет
- Lecture 4 Individual Statutory Rights Affecting The Course of Employment Lecture VersionДокумент51 страницаLecture 4 Individual Statutory Rights Affecting The Course of Employment Lecture VersionNg Yih MiinОценок пока нет
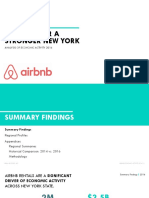
- Airbnb Economic Activity Report, New York State HR&AДокумент37 страницAirbnb Economic Activity Report, New York State HR&ARyan WhalenОценок пока нет
- Keyur PrajapatiДокумент66 страницKeyur PrajapatiAyush JainОценок пока нет
- MinacsДокумент1 страницаMinacsudi969Оценок пока нет
- B2 Grammar Test 1Документ4 страницыB2 Grammar Test 1steadyfalconОценок пока нет
- ICAB Certificate Level Taxation Nov 17Документ9 страницICAB Certificate Level Taxation Nov 17Prithvi PrasadОценок пока нет
- ACCT 102 Lecture Notes Chapter 15 SPR 2016Документ4 страницыACCT 102 Lecture Notes Chapter 15 SPR 2016xenoyewОценок пока нет
- Corporate Finance 1Документ340 страницCorporate Finance 1tieuma712Оценок пока нет