Вам также может понравиться
- Documentation of Medical RecordsДокумент51 страницаDocumentation of Medical Recordsalwy aliОценок пока нет
- Documentation for Skilled Nursing & Long-Term Care: A Guide for Occupational TherapistsОт EverandDocumentation for Skilled Nursing & Long-Term Care: A Guide for Occupational TherapistsОценок пока нет
- The Problem Oriented Medical RecordДокумент32 страницыThe Problem Oriented Medical RecordPriscila TanuwidjajaОценок пока нет
- Textbook of Urgent Care Management: Chapter 16, Urgent Care Duties, Staffing Mix and RatiosОт EverandTextbook of Urgent Care Management: Chapter 16, Urgent Care Duties, Staffing Mix and RatiosОценок пока нет
- Documentation & Reporting in Nursing - EFNДокумент4 страницыDocumentation & Reporting in Nursing - EFNadellia onyОценок пока нет
- NursingДокумент57 страницNursingremzylicious100% (1)
- Textbook of Urgent Care Management: Chapter 42, Evaluation and Management of Coding and DocumentationОт EverandTextbook of Urgent Care Management: Chapter 42, Evaluation and Management of Coding and DocumentationОценок пока нет
- DocumentationДокумент15 страницDocumentationAra- Cvsu Francisco100% (2)
- Unit 1 Documentation-and-ReportingДокумент39 страницUnit 1 Documentation-and-ReportingMs.V. Mahesha Asst. Prof.Оценок пока нет
- Documentation: Basic Nursing: Foundations of Skills & Concepts DocumentationДокумент8 страницDocumentation: Basic Nursing: Foundations of Skills & Concepts DocumentationJona GarzonОценок пока нет
- Newman's Certified Electronic Health Records Technician Study GuideОт EverandNewman's Certified Electronic Health Records Technician Study GuideОценок пока нет
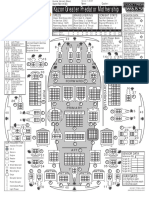
- Kazon Greater Predator MothershipДокумент1 страницаKazon Greater Predator MothershipknavealphaОценок пока нет
- Maintenance of Records and ReportsДокумент81 страницаMaintenance of Records and ReportsSanjna Kumari (SNSR Senior Tutor/Lecturer)100% (1)
- Week 13 Documentation in Psychiatric Mental Health Nursing PracticeДокумент69 страницWeek 13 Documentation in Psychiatric Mental Health Nursing PracticeJeff MalinisОценок пока нет
- Patients Medical ChartДокумент25 страницPatients Medical ChartErlyn EnocОценок пока нет
- NICU Documentation: Gama Hospital Al Khobar K.S.AДокумент8 страницNICU Documentation: Gama Hospital Al Khobar K.S.ALucian CaelumОценок пока нет
- Lesson 1-Documentation and ReportingДокумент8 страницLesson 1-Documentation and ReportingCHRISTIAN ROY MAXINO100% (1)
- Nursing Record and ReportsДокумент32 страницыNursing Record and ReportsOm VaishNav100% (1)
- 2022 Mable Parker Mclean Scholarship ApplicationДокумент2 страницы2022 Mable Parker Mclean Scholarship Applicationapi-444959661Оценок пока нет
- Medical Record Department: Ravi Bagali Jayendra Tripati Amrithayan Das Shivaram Gaurav RaviДокумент61 страницаMedical Record Department: Ravi Bagali Jayendra Tripati Amrithayan Das Shivaram Gaurav RaviRashid AyubiОценок пока нет
- Nursing Process and DocumentationДокумент52 страницыNursing Process and Documentationgeorgeloto12100% (2)
- Sources of Hindu LawДокумент9 страницSources of Hindu LawKrishnaKousikiОценок пока нет
- (1921) Manual of Work Garment Manufacture: How To Improve Quality and Reduce CostsДокумент102 страницы(1921) Manual of Work Garment Manufacture: How To Improve Quality and Reduce CostsHerbert Hillary Booker 2nd100% (1)
- Charting (Sample)Документ9 страницCharting (Sample)Zarah Joy Tabuyan100% (3)
- Types of Medical RecordsДокумент17 страницTypes of Medical RecordsPriyanka Roy Chowdhury57% (7)
- Nicu DoccumentationДокумент17 страницNicu Doccumentationchaarvi100% (1)
- 1.1 Background Nursing Documentation Is The Record of Nursing Care That Is Planned and Delivered ToДокумент13 страниц1.1 Background Nursing Documentation Is The Record of Nursing Care That Is Planned and Delivered Toari cendani prabawatiОценок пока нет
- Nursing ProcessДокумент52 страницыNursing ProcessDzon LornaОценок пока нет
- Documentation in NursingДокумент41 страницаDocumentation in NursingGLAIZA PALATINOОценок пока нет
- Documentation System Focus ChartingДокумент26 страницDocumentation System Focus ChartingneehoshiОценок пока нет
- Records and ReportДокумент4 страницыRecords and ReportAnusikta PandaОценок пока нет
- 9 3 2012 Charting and DocumentationДокумент44 страницы9 3 2012 Charting and DocumentationMacrossBalaОценок пока нет
- Documenting and ReportingДокумент17 страницDocumenting and ReportingalelichengОценок пока нет
- Documentation 2016Документ52 страницыDocumentation 2016jenОценок пока нет
- NapulanRM - Health Records Analysis and Clinical AuditДокумент64 страницыNapulanRM - Health Records Analysis and Clinical AuditJeffreyReyesОценок пока нет
- AssessmentДокумент32 страницыAssessmentAubrey MitraОценок пока нет
- Changing Mainline IV BagДокумент5 страницChanging Mainline IV BagLorna PaghunasanОценок пока нет
- Focus Charting at North Bay General Hospital DAEДокумент67 страницFocus Charting at North Bay General Hospital DAECzarina GuintoОценок пока нет
- Documentation and Informatics in NursingДокумент34 страницыDocumentation and Informatics in NursingHaneen Jehad Um MalekОценок пока нет
- Nursing Documentation1Документ3 страницыNursing Documentation1Paskuman DinkesОценок пока нет
- Sparks Taylors Nursing Diagnosis Pocket Guide 3rd Edition Ebook PDFДокумент61 страницаSparks Taylors Nursing Diagnosis Pocket Guide 3rd Edition Ebook PDFzelma.bennett128100% (42)
- Documentation & Reporting in Nursing: PurposesДокумент5 страницDocumentation & Reporting in Nursing: PurposesMeike ElfkyuminMvp's BanabestfriendmelodyОценок пока нет
- Medical RecordsДокумент331 страницаMedical Recordssgekara cyberОценок пока нет
- Midterms - HA LabДокумент17 страницMidterms - HA LabMa. Daniela De la CernaОценок пока нет
- Chapter 1 The Accident and ImergencyДокумент35 страницChapter 1 The Accident and ImergencyKusumadewi WidiarsaОценок пока нет
- Documentation For NursesДокумент6 страницDocumentation For NursesJanine AndersonОценок пока нет
- Nursing DiagnosisДокумент38 страницNursing DiagnosisJR Rolf NeuqeletОценок пока нет
- Documentation: VN230 Vocational Nursing Spring 2007Документ44 страницыDocumentation: VN230 Vocational Nursing Spring 2007brendz_pontelaОценок пока нет
- HA-Midterms LabДокумент13 страницHA-Midterms LabMa. Daniela De la CernaОценок пока нет
- Recording Training: General ObjectiveДокумент8 страницRecording Training: General ObjectiveFarida ZakzoukОценок пока нет
- Group11 MOPДокумент5 страницGroup11 MOPjilliantrcieОценок пока нет
- (Nursing English) DIYAH AHADYATUNNISAДокумент10 страниц(Nursing English) DIYAH AHADYATUNNISAdiyah hansuОценок пока нет
- Documenting and ReportingДокумент5 страницDocumenting and ReportingElla LobenariaОценок пока нет
- FARM Note CarePlansДокумент11 страницFARM Note CarePlansbrain bareОценок пока нет
- Documentationand Nursing InformaticsДокумент36 страницDocumentationand Nursing Informaticsharley dela cruzОценок пока нет
- Kami Ridho Allah SWT Sebagai Tuhanku, Islam Sebagai Agamaku, Dan Nabi Muhammad Sebagai Nabi Dan Rasul, Ya Allah, Tambahkanlah Kepadaku Ilmu Dan Berikanlah Aku KefahamanДокумент65 страницKami Ridho Allah SWT Sebagai Tuhanku, Islam Sebagai Agamaku, Dan Nabi Muhammad Sebagai Nabi Dan Rasul, Ya Allah, Tambahkanlah Kepadaku Ilmu Dan Berikanlah Aku Kefahamanalif kuncorojatiОценок пока нет
- 1 Client Records 1Документ15 страниц1 Client Records 1Grape JuiceОценок пока нет
- Legal Protection of Nursing ServiceДокумент4 страницыLegal Protection of Nursing ServiceJanna Kristine Ferrer Yosores80% (5)
- Healthcare ProjectДокумент13 страницHealthcare ProjectDivyansh SrivastavaОценок пока нет
- NCM-101 - Module-7 - 2Документ39 страницNCM-101 - Module-7 - 2Princess Javier TorcelinoОценок пока нет
- Documentation Documentation of Patient Teaching Characteristics of Documentation Components of DocumentationДокумент10 страницDocumentation Documentation of Patient Teaching Characteristics of Documentation Components of DocumentationLira MacoОценок пока нет
- Documentation and ReportingДокумент51 страницаDocumentation and ReportingYsabella LlanetaОценок пока нет
- Holycrosscollege of Nursing Kottiyam, Kollam: I B Sc. NURSING STUDENTS - 2018-2019 (XV Batch)Документ5 страницHolycrosscollege of Nursing Kottiyam, Kollam: I B Sc. NURSING STUDENTS - 2018-2019 (XV Batch)Praveen ThulasiОценок пока нет
- Osmosis Is The Movement of Water Across Cell Membranes, From The Less ConcentratedДокумент1 страницаOsmosis Is The Movement of Water Across Cell Membranes, From The Less ConcentratedPraveen ThulasiОценок пока нет
- Curriculum Vitae: Bincy RajДокумент3 страницыCurriculum Vitae: Bincy RajPraveen ThulasiОценок пока нет
- Sree Gokulam Nursing College: SPRINT 2014Документ1 страницаSree Gokulam Nursing College: SPRINT 2014Praveen ThulasiОценок пока нет
- Mechanical Ventilation: Essentials For Registered NursesДокумент49 страницMechanical Ventilation: Essentials For Registered NursesPraveen ThulasiОценок пока нет
- Life Skill - D: EfinitionДокумент16 страницLife Skill - D: EfinitionPraveen ThulasiОценок пока нет
- Sree Gokulam Nursing College: Department of Mental Health NursingДокумент3 страницыSree Gokulam Nursing College: Department of Mental Health NursingPraveen ThulasiОценок пока нет
- Bom Details FormatДокумент6 страницBom Details FormatPrince MittalОценок пока нет
- Winter CrocFest 2017 at St. Augustine Alligator Farm - Final ReportДокумент6 страницWinter CrocFest 2017 at St. Augustine Alligator Farm - Final ReportColette AdamsОценок пока нет
- Bolt Grade Markings and Strength ChartДокумент2 страницыBolt Grade Markings and Strength ChartGregory GaschteffОценок пока нет
- Topic 3Документ21 страницаTopic 3Ivan SimonОценок пока нет
- Bullshit System v0.5Документ40 страницBullshit System v0.5ZolaniusОценок пока нет
- Peer PressureДокумент13 страницPeer PressuremightymarcОценок пока нет
- What Are The Spacer Bars in RC Beams - QuoraДокумент3 страницыWhat Are The Spacer Bars in RC Beams - QuoradesignОценок пока нет
- Close Enough To Touch by Victoria Dahl - Chapter SamplerДокумент23 страницыClose Enough To Touch by Victoria Dahl - Chapter SamplerHarlequinAustraliaОценок пока нет
- Government College of Nursing Jodhpur: Practice Teaching On-Probability Sampling TechniqueДокумент11 страницGovernment College of Nursing Jodhpur: Practice Teaching On-Probability Sampling TechniquepriyankaОценок пока нет
- 1 in 8.5 60KG PSC Sleepers TurnoutДокумент9 страниц1 in 8.5 60KG PSC Sleepers Turnoutrailway maintenanceОценок пока нет
- Hướng Dẫn Chấm: Ngày thi: 27 tháng 7 năm 2019 Thời gian làm bài: 180 phút (không kể thời gian giao đề) HDC gồm có 4 trangДокумент4 страницыHướng Dẫn Chấm: Ngày thi: 27 tháng 7 năm 2019 Thời gian làm bài: 180 phút (không kể thời gian giao đề) HDC gồm có 4 trangHưng Quân VõОценок пока нет
- Lecture 2 Effects of Operating Conditions in VCCДокумент9 страницLecture 2 Effects of Operating Conditions in VCCDeniell Joyce MarquezОценок пока нет
- Subject Manual Tle 7-8Документ11 страницSubject Manual Tle 7-8Rhayan Dela Cruz DaquizОценок пока нет
- Delonghi Esam Series Service Info ItalyДокумент10 страницDelonghi Esam Series Service Info ItalyBrko BrkoskiОценок пока нет
- Miguel Augusto Ixpec-Chitay, A097 535 400 (BIA Sept. 16, 2013)Документ22 страницыMiguel Augusto Ixpec-Chitay, A097 535 400 (BIA Sept. 16, 2013)Immigrant & Refugee Appellate Center, LLCОценок пока нет
- My Mother at 66Документ6 страницMy Mother at 66AnjanaОценок пока нет
- An Evaluation of MGNREGA in SikkimДокумент7 страницAn Evaluation of MGNREGA in SikkimBittu SubbaОценок пока нет
- Genetics Icar1Документ18 страницGenetics Icar1elanthamizhmaranОценок пока нет
- Julia Dito ResumeДокумент3 страницыJulia Dito Resumeapi-253713289Оценок пока нет
- Literatura Tecnica 3Документ10 страницLiteratura Tecnica 3Christian PerezОценок пока нет
- ReadmeДокумент2 страницыReadmechethan100% (1)
- Presentation About GyroscopesДокумент24 страницыPresentation About GyroscopesgeenjunkmailОценок пока нет
- Fds-Ofite Edta 0,1MДокумент7 страницFds-Ofite Edta 0,1MVeinte Años Sin VosОценок пока нет
- Where We Are in Place and Time "We Are Part of The Universe and Feel Compelled To Explore It."Документ1 страницаWhere We Are in Place and Time "We Are Part of The Universe and Feel Compelled To Explore It."Safia-umm Suhaim- FareedОценок пока нет
- Catedral de SevillaДокумент28 страницCatedral de SevillaAnonymous LkgNmKeОценок пока нет
- Sample - SOFTWARE REQUIREMENT SPECIFICATIONДокумент20 страницSample - SOFTWARE REQUIREMENT SPECIFICATIONMandula AbeyrathnaОценок пока нет