Вам также может понравиться
- Jpts 26 855Документ2 страницыJpts 26 855Yoga MatiinuОценок пока нет
- Effects of Proprioceptive Neuromuscular Facilitation Stretching and Kinesiology Taping On Pelvic Compensation During Double-Knee ExtensionДокумент10 страницEffects of Proprioceptive Neuromuscular Facilitation Stretching and Kinesiology Taping On Pelvic Compensation During Double-Knee ExtensionElan R.S.Оценок пока нет
- Accepted ManuscriptДокумент40 страницAccepted ManuscriptDaniel CarcamoОценок пока нет
- Dickie 2016Документ28 страницDickie 2016FranciscoОценок пока нет
- Low Back Joint Loading and Kinematics During Standing and Unsupported SittingДокумент17 страницLow Back Joint Loading and Kinematics During Standing and Unsupported SittingDandy DharmaОценок пока нет
- CallaghanДокумент16 страницCallaghanhenry EkwuemeОценок пока нет
- An Electromyographic Analysis of Trunk and Hip Extensor Muscles During Bridging Exercises - Effect of Voluntary Control of The Pelvic TiltДокумент3 страницыAn Electromyographic Analysis of Trunk and Hip Extensor Muscles During Bridging Exercises - Effect of Voluntary Control of The Pelvic TiltNicolás ManonniОценок пока нет
- Acute Effects of Hamstring Stretching On Sagittal Spinal Curvatures and Pelvic TiltДокумент10 страницAcute Effects of Hamstring Stretching On Sagittal Spinal Curvatures and Pelvic TiltOcAn D'scAmpОценок пока нет
- E F T S E - M D: AP S: Ffect of Lexibility Raining On Ymptoms OF Xercise Induced Uscle Amage Reliminary TudyДокумент7 страницE F T S E - M D: AP S: Ffect of Lexibility Raining On Ymptoms OF Xercise Induced Uscle Amage Reliminary TudySudhakar SubramanianОценок пока нет
- Emg Deltoide Diferentes Exercicios Silveira Lima 2013 PDFДокумент5 страницEmg Deltoide Diferentes Exercicios Silveira Lima 2013 PDFAlexandreОценок пока нет
- Effects of Fatigue On Stability of Upper Extremity During Bench-Press ExerciseДокумент5 страницEffects of Fatigue On Stability of Upper Extremity During Bench-Press Exerciseyp huangОценок пока нет
- The Effect of Thoracic Spine MobilizationДокумент4 страницыThe Effect of Thoracic Spine MobilizationEric SimasОценок пока нет
- Effect of Isometric Horizontal Abduction On Pectoralis Major and Serratus AnteriorДокумент7 страницEffect of Isometric Horizontal Abduction On Pectoralis Major and Serratus AnteriorRudolfGerОценок пока нет
- Brazilian Journal of Physical TherapyДокумент10 страницBrazilian Journal of Physical TherapyLuis DavidОценок пока нет
- Abb2017 9084725Документ8 страницAbb2017 9084725Gonzalo GonzalesОценок пока нет
- PT Journal Musclel ActivityДокумент8 страницPT Journal Musclel ActivityKarthigaMurugesanОценок пока нет
- An Electromyographic Analysis of Trunk and Hip Extensor Muscles During Bridging Exercises - Effect of Voluntary Control of The Pelvic TiltДокумент3 страницыAn Electromyographic Analysis of Trunk and Hip Extensor Muscles During Bridging Exercises - Effect of Voluntary Control of The Pelvic TiltNicolás ManonniОценок пока нет
- Activation and Torque Deficits in ACL-Reconstructed Patients 4 Months Post-OperativeДокумент15 страницActivation and Torque Deficits in ACL-Reconstructed Patients 4 Months Post-OperativeEurovision RSОценок пока нет
- (534816417) DownloadДокумент7 страниц(534816417) Downloadpito12Оценок пока нет
- 2010 - Manual Therapy PDFДокумент5 страниц2010 - Manual Therapy PDFYuzo IgarashiОценок пока нет
- Obesity CuadricepsДокумент5 страницObesity CuadricepsGonzalo Aguayo AlcayagaОценок пока нет
- Glut MedMaxДокумент12 страницGlut MedMaxColm CoakleyОценок пока нет
- Muscle Activation and Local Muscular Fatigue During A 12-Minute Rotational BridgeДокумент13 страницMuscle Activation and Local Muscular Fatigue During A 12-Minute Rotational BridgeadindaОценок пока нет
- Manual Therapy: Original ArticleДокумент5 страницManual Therapy: Original ArticleCleber PimentaОценок пока нет
- The Effect of Different Decline Angles On The Biomechanics of Double Limb Squats and The Implications To Clinical and Training PracticeДокумент15 страницThe Effect of Different Decline Angles On The Biomechanics of Double Limb Squats and The Implications To Clinical and Training Practicesebastian floresОценок пока нет
- J Jelekin 2014 06 002 PDFДокумент38 страницJ Jelekin 2014 06 002 PDFRommel AndresОценок пока нет
- SciДокумент9 страницSciCathyCarltonОценок пока нет
- Effects of Respiratory-Muscle Exercise On Spinal CurvatureДокумент6 страницEffects of Respiratory-Muscle Exercise On Spinal CurvatureChrisОценок пока нет
- Articulo #30Документ8 страницArticulo #30LAURA CAMILA CUBILLOS VILLAMILОценок пока нет
- High-Intensity Running and Plantar-Flexor Fatigability and Plantar-Pressure Distribution in Adolescent RunnersДокумент9 страницHigh-Intensity Running and Plantar-Flexor Fatigability and Plantar-Pressure Distribution in Adolescent Runnersflx.vernetОценок пока нет
- Range of Motion and Leg Rotation Affect EMG Activation Levels of The Superficial Quadriceps Muscles During Leg Extension.Документ11 страницRange of Motion and Leg Rotation Affect EMG Activation Levels of The Superficial Quadriceps Muscles During Leg Extension.Ticinosthetics GainzSchoolОценок пока нет
- Artigo AfundoДокумент23 страницыArtigo AfundoYan MatosОценок пока нет
- Home-Based - Electromyography-TrДокумент10 страницHome-Based - Electromyography-Trjorgequintero927470Оценок пока нет
- Hamstring OM 21Документ5 страницHamstring OM 21Dr Ahmed NabilОценок пока нет
- Hamstring 3Документ4 страницыHamstring 3Ardhyan ArdhyanОценок пока нет
- Sms 13770Документ29 страницSms 13770Peio KominoОценок пока нет
- Ipsilateral Hip Abductor Weakness After Inversion Ankle SprainДокумент5 страницIpsilateral Hip Abductor Weakness After Inversion Ankle SprainZmajОценок пока нет
- Ejercicios Cadera TroncoДокумент9 страницEjercicios Cadera TroncoNicol Jerez ParraОценок пока нет
- Muscle Activation Pattern of Hip Arthroplasty Patients in WalkingДокумент9 страницMuscle Activation Pattern of Hip Arthroplasty Patients in Walkingsebas valadezОценок пока нет
- Exaggerated Interlimb Neural Coupling Following Stroke: Tiffany L. Kline, Brian D. Schmit and Derek G. KamperДокумент11 страницExaggerated Interlimb Neural Coupling Following Stroke: Tiffany L. Kline, Brian D. Schmit and Derek G. KamperArup KuntiОценок пока нет
- Changes in Postural Stability With Fatigue of Lower Extremity Frontal and Sagittal Plane MoversДокумент5 страницChanges in Postural Stability With Fatigue of Lower Extremity Frontal and Sagittal Plane MoversKhaled AbuzayanОценок пока нет
- How Long Does The Protective Effect On Eccentric Exercise-Induced Muscle Damage Last?Документ6 страницHow Long Does The Protective Effect On Eccentric Exercise-Induced Muscle Damage Last?Ricardo Pereira NevesОценок пока нет
- Hip-Abductor Fatigue, Frontal-Plane Landing Angle, and Excursion During A Drop JumpДокумент11 страницHip-Abductor Fatigue, Frontal-Plane Landing Angle, and Excursion During A Drop JumpIlham MaulanaОценок пока нет
- Effects of Kinesiology Taping On Repositioning Error of The Knee Joint After Quadriceps Muscle FatigueДокумент3 страницыEffects of Kinesiology Taping On Repositioning Error of The Knee Joint After Quadriceps Muscle FatigueYoga MatiinuОценок пока нет
- Análise EMG de Músculos Das Extremidades Inferiores em Três Diferentes Exercícios de AgachamentoДокумент6 страницAnálise EMG de Músculos Das Extremidades Inferiores em Três Diferentes Exercícios de AgachamentoSheilani MartinsОценок пока нет
- Differences in Muscle Shoulder External Rotation in Open Kinetic Chain and Closed Kinetic Chain Exercises PDFДокумент3 страницыDifferences in Muscle Shoulder External Rotation in Open Kinetic Chain and Closed Kinetic Chain Exercises PDFLeonardiniОценок пока нет
- December2006RRHardwickДокумент8 страницDecember2006RRHardwickHaile Mariam González GarcíaОценок пока нет
- Positive Force Feedback in Human WalkingДокумент8 страницPositive Force Feedback in Human Walkingfernando_a_gonzalezОценок пока нет
- Effects of Squat Training With Different Depths On Lower Limb Muscle VolumesДокумент10 страницEffects of Squat Training With Different Depths On Lower Limb Muscle VolumesjoselucasspОценок пока нет
- Gefen Et Al. - 2002 - Analysis of Muscular Fatigue and Foot Stability During High-Heeled GaitДокумент8 страницGefen Et Al. - 2002 - Analysis of Muscular Fatigue and Foot Stability During High-Heeled GaitAwatef FituriОценок пока нет
- 13 Marchetti 380 384pulloverДокумент6 страниц13 Marchetti 380 384pullovercderosasОценок пока нет
- Reduced Plantar Sensation Causes A Cautious Walking Pattern: Cite This PaperДокумент9 страницReduced Plantar Sensation Causes A Cautious Walking Pattern: Cite This PaperAhmed AllamОценок пока нет
- Reactive Balance Adjustments To UnexpectДокумент11 страницReactive Balance Adjustments To UnexpectergoshaunОценок пока нет
- Spinal Myo After InjuryДокумент12 страницSpinal Myo After InjuryVincentius Michael WilliantoОценок пока нет
- 2015 - Chronic Neck Pain Alters Muscle Activation Patterns To Sudden Movements (D. Falla)Документ11 страниц2015 - Chronic Neck Pain Alters Muscle Activation Patterns To Sudden Movements (D. Falla)romiromiromi123Оценок пока нет
- Muscle Activation and Kinematic Analysis During The Inclined Leg Press Exercise in Young FemalesДокумент14 страницMuscle Activation and Kinematic Analysis During The Inclined Leg Press Exercise in Young FemalesMari Calica GimenezОценок пока нет
- 23 247Документ4 страницы23 247Ita MagdalenaОценок пока нет
- Analysis of The Hamstring Muscle Activation During Two Injury Prevention ExercisesДокумент9 страницAnalysis of The Hamstring Muscle Activation During Two Injury Prevention ExercisesJoeОценок пока нет
- Length Tension Testing Book 1, Lower Quadrant: A Workbook of Manual Therapy TechniquesОт EverandLength Tension Testing Book 1, Lower Quadrant: A Workbook of Manual Therapy TechniquesРейтинг: 3.5 из 5 звезд3.5/5 (3)
- Principles of Manual Medicine for Sacroiliac Joint Dysfunction: Arthrokinematic Approach-Hakata MethodОт EverandPrinciples of Manual Medicine for Sacroiliac Joint Dysfunction: Arthrokinematic Approach-Hakata MethodShigehiko KatadaОценок пока нет
- 2 Saunders00thebarbersunhappinessДокумент20 страниц2 Saunders00thebarbersunhappinessCharlie HigginsОценок пока нет
- 1 Englander99thetwentyseventhmanДокумент13 страниц1 Englander99thetwentyseventhmanCharlie HigginsОценок пока нет
- 2 Nabokov95scenesfromthelifeofadoublemonsterДокумент5 страниц2 Nabokov95scenesfromthelifeofadoublemonsterCharlie HigginsОценок пока нет
- AcharyaPK ArchitectureOfManasaraTranslationДокумент246 страницAcharyaPK ArchitectureOfManasaraTranslationCharlie Higgins67% (3)
- Reade MilkingCheeseSealДокумент3 страницыReade MilkingCheeseSealCharlie HigginsОценок пока нет
- 2 Horrocks06embodiedДокумент9 страниц2 Horrocks06embodiedCharlie HigginsОценок пока нет
- Roth LegendsOfCraftsmenInJainaLiteratureДокумент19 страницRoth LegendsOfCraftsmenInJainaLiteratureCharlie HigginsОценок пока нет
- Technique of Wood Work - Some References in Ancient IndiaДокумент3 страницыTechnique of Wood Work - Some References in Ancient IndiaCharlie HigginsОценок пока нет
- Anschuetz Et Al 2001 - An Archaeology of Landscapes, Perspectives and DirectionsДокумент56 страницAnschuetz Et Al 2001 - An Archaeology of Landscapes, Perspectives and DirectionsNagy József GáborОценок пока нет
- Everyday Life in Babylon and AssyriaДокумент8 страницEveryday Life in Babylon and AssyriaCharlie HigginsОценок пока нет
- MilkingBhagavata (Fromgray)Документ1 страницаMilkingBhagavata (Fromgray)Charlie HigginsОценок пока нет
- James EgyptianPaintingAndDrawingДокумент10 страницJames EgyptianPaintingAndDrawingCharlie HigginsОценок пока нет
- Dellovin ACarpenter'sToolKitCentralWesternIranДокумент27 страницDellovin ACarpenter'sToolKitCentralWesternIranCharlie HigginsОценок пока нет
- Technique of Wood Work - Some References in Ancient IndiaДокумент3 страницыTechnique of Wood Work - Some References in Ancient IndiaCharlie HigginsОценок пока нет
- Brouwer SouthIndianBlacksmithAndGoldsmithДокумент14 страницBrouwer SouthIndianBlacksmithAndGoldsmithCharlie HigginsОценок пока нет
- Tamil Writing 1672Документ2 страницыTamil Writing 1672Charlie HigginsОценок пока нет
- Dehejia RepresentingBodyGenderIssuesIndianArt PDFДокумент37 страницDehejia RepresentingBodyGenderIssuesIndianArt PDFCharlie Higgins50% (2)
- Brouwer SouthIndianBlacksmithAndGoldsmithДокумент14 страницBrouwer SouthIndianBlacksmithAndGoldsmithCharlie HigginsОценок пока нет
- Waele EtchedCarnelianBeadsFromNESEArabiaДокумент10 страницWaele EtchedCarnelianBeadsFromNESEArabiaCharlie HigginsОценок пока нет
- Calcutta School 1825Документ2 страницыCalcutta School 1825Charlie HigginsОценок пока нет
- Ergas ReligionAndBodyReclaimingMissingLinksWesternEducationДокумент12 страницErgas ReligionAndBodyReclaimingMissingLinksWesternEducationCharlie HigginsОценок пока нет
- Ostor FilmingInNayaVillageДокумент5 страницOstor FilmingInNayaVillageCharlie HigginsОценок пока нет
- Charleston - Wheel Engraving and Cutting Some Early EquipmentДокумент18 страницCharleston - Wheel Engraving and Cutting Some Early EquipmentCharlie HigginsОценок пока нет
- Ergas ReligionAndBodyReclaimingMissingLinksWesternEducationДокумент12 страницErgas ReligionAndBodyReclaimingMissingLinksWesternEducationCharlie HigginsОценок пока нет
- Veda Teaching FrogsДокумент4 страницыVeda Teaching FrogsCharlie HigginsОценок пока нет
- Eguchi MusicAndReligionOfDiasporicIndiansInPittsburgДокумент116 страницEguchi MusicAndReligionOfDiasporicIndiansInPittsburgCharlie HigginsОценок пока нет
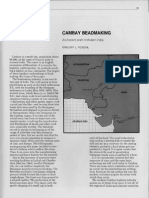
- Possehl CambayBeadmakingДокумент5 страницPossehl CambayBeadmakingCharlie HigginsОценок пока нет
- Ostor FilmingInNayaVillageДокумент5 страницOstor FilmingInNayaVillageCharlie HigginsОценок пока нет
- Wrightetal2008 LevantДокумент35 страницWrightetal2008 LevantVíctor M GonzálezОценок пока нет
- Meyer SexualLifeInAncientIndiaДокумент616 страницMeyer SexualLifeInAncientIndiaCharlie HigginsОценок пока нет
- SampleДокумент13 страницSamplemypermatakoe71Оценок пока нет
- BTech ORB40PT 2014 Study Guide - V3Документ41 страницаBTech ORB40PT 2014 Study Guide - V3Khosi GrootboomОценок пока нет
- Analytical ExpositionДокумент7 страницAnalytical ExpositionEman FakotОценок пока нет
- Valve Type Trim Type CF XTДокумент1 страницаValve Type Trim Type CF XTAye KyweОценок пока нет
- Steam Circulation SystemДокумент36 страницSteam Circulation Systemjkhan_724384100% (1)
- Maintenance Manual - Booms: S Booms Z BoomsДокумент185 страницMaintenance Manual - Booms: S Booms Z BoomsRafael Vieira De AssisОценок пока нет
- 4MA1 1H Que 20210304Документ28 страниц4MA1 1H Que 20210304mo gaОценок пока нет
- Scheme of Examination For Master of Computer APPLICATIONS (M.C.A.) W.E.F. Academic Session 2014-15Документ11 страницScheme of Examination For Master of Computer APPLICATIONS (M.C.A.) W.E.F. Academic Session 2014-15Siddharth JainОценок пока нет
- Ethics PresentationДокумент2 страницыEthics PresentationAbhinavGuptaОценок пока нет
- The Jambeli Culture of South Coastal Ecuador Estrada Meggers y EvansДокумент93 страницыThe Jambeli Culture of South Coastal Ecuador Estrada Meggers y EvansMarco VargasОценок пока нет
- QUANTUM TELEPORTATIONДокумент23 страницыQUANTUM TELEPORTATIONalkagabaОценок пока нет
- Particulate Contamination in Aviation Fuels by Laboratory FiltrationДокумент11 страницParticulate Contamination in Aviation Fuels by Laboratory FiltrationMuhammad KhairuddinОценок пока нет
- Student's Guide To Year 9 and 10 Science (Stage 5)Документ38 страницStudent's Guide To Year 9 and 10 Science (Stage 5)dan964100% (1)
- DLL Theorems On RectangleДокумент5 страницDLL Theorems On RectanglePatrick Guerra100% (1)
- Texts Hugues de VarineДокумент15 страницTexts Hugues de VarineInteractionsonlineОценок пока нет
- Speech and Modes of SpeechДокумент27 страницSpeech and Modes of SpeechShaira MejaresОценок пока нет
- FRS - Brake System - TrainsetДокумент12 страницFRS - Brake System - TrainsetCad TutorОценок пока нет
- CED-2021 EnergyTransition ReportДокумент75 страницCED-2021 EnergyTransition ReportCityNewsTorontoОценок пока нет
- What Is A BibliographyДокумент7 страницWhat Is A BibliographyKaye Diamante ValleserОценок пока нет
- ClassДокумент40 страницClassapi-449920999Оценок пока нет
- Expansion Joint Treatment Materials and TechniquesДокумент15 страницExpansion Joint Treatment Materials and TechniquesMAHAK GUPTAОценок пока нет
- Clearings 2018Документ22 страницыClearings 2018ldxb2001100% (1)
- 574-Article Text-1139-1-10-20170930Документ12 страниц574-Article Text-1139-1-10-20170930Jhufry GhanterОценок пока нет
- Calibration Procedure Crowcon Xgard Gas Detectors - 5720273 - 01Документ16 страницCalibration Procedure Crowcon Xgard Gas Detectors - 5720273 - 01Daniel Rolando Gutierrez FuentesОценок пока нет
- MSDS Chrome Catalyst Safety SheetДокумент4 страницыMSDS Chrome Catalyst Safety Sheetstavros7Оценок пока нет
- Iso 9712 2012 PDFДокумент19 страницIso 9712 2012 PDFBala KrishnanОценок пока нет
- Manifest Merger Debug ReportДокумент14 страницManifest Merger Debug ReportRam PankhaniyaОценок пока нет
- MFS 7104 Quantitative TechniquesДокумент2 страницыMFS 7104 Quantitative TechniquesDavid KОценок пока нет
- Three Theories of TruthДокумент1 страницаThree Theories of TruthDn AngelОценок пока нет
- Quote: Quotation Prepared By: Sloan SellersДокумент2 страницыQuote: Quotation Prepared By: Sloan SellersRubén CastañoОценок пока нет