Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Drew Marine Chemical ManualДокумент36 страницDrew Marine Chemical ManualcpiquiОценок пока нет
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Soil Mechanics Lecture 1Документ86 страницSoil Mechanics Lecture 1Ammar Ayub100% (2)
- Skeletal TraumaДокумент56 страницSkeletal Traumag1381821Оценок пока нет
- Git LymphomasДокумент43 страницыGit Lymphomasg1381821Оценок пока нет
- Thyroid MalignancyДокумент65 страницThyroid Malignancyg1381821Оценок пока нет
- Concepts of Radiologic ScienceДокумент57 страницConcepts of Radiologic Scienceg1381821Оценок пока нет
- Diffrential Diagnosis of Gastric Masses and NarrowingДокумент62 страницыDiffrential Diagnosis of Gastric Masses and Narrowingg1381821Оценок пока нет
- Intestinal Obstruction in ChildrenДокумент63 страницыIntestinal Obstruction in Childreng1381821Оценок пока нет
- Radiographic FILMДокумент54 страницыRadiographic FILMg1381821Оценок пока нет
- The Urethra and Male Genital TractДокумент70 страницThe Urethra and Male Genital Tractg1381821Оценок пока нет
- Ultrasound Guided ProceduresДокумент71 страницаUltrasound Guided Proceduresg1381821Оценок пока нет
- Pulmonary HypertensionДокумент43 страницыPulmonary Hypertensiong1381821Оценок пока нет
- Breast UltrasoundДокумент46 страницBreast Ultrasoundg138182175% (4)
- Health PhysicsДокумент33 страницыHealth Physicsg1381821Оценок пока нет
- Case Presentation: Radiology HMCДокумент78 страницCase Presentation: Radiology HMCg1381821Оценок пока нет
- Brain IschemiaДокумент43 страницыBrain Ischemiag1381821Оценок пока нет
- Case Presentation: DR Tariq Masood TMO Radiology Department, HMCДокумент82 страницыCase Presentation: DR Tariq Masood TMO Radiology Department, HMCg1381821Оценок пока нет
- Radiation Hazards and Its Protection: DR - Rabia ShahДокумент43 страницыRadiation Hazards and Its Protection: DR - Rabia Shahg13818210% (1)
- Paediatric Abdominal MassesДокумент73 страницыPaediatric Abdominal Massesg1381821Оценок пока нет
- Infant Cranial UltrasoundДокумент73 страницыInfant Cranial Ultrasoundg1381821100% (1)
- Radiology Department Hayat Abad Medical ComplexДокумент24 страницыRadiology Department Hayat Abad Medical Complexg1381821Оценок пока нет
- Excretory UrographyДокумент64 страницыExcretory Urographyg1381821Оценок пока нет
- The Role of Ultrasound in Obstetric and GynaecologyДокумент9 страницThe Role of Ultrasound in Obstetric and Gynaecologyg1381821Оценок пока нет
- Medical Devices On The Chest X RayДокумент114 страницMedical Devices On The Chest X Rayg1381821Оценок пока нет
- Diagnostic Ultrasound For Postgraduates in ObstetricsДокумент33 страницыDiagnostic Ultrasound For Postgraduates in Obstetricsg1381821Оценок пока нет
- Hypertrophic Pyloric Stenosis Tips and Tricks For Ultrasound DiagnosisДокумент4 страницыHypertrophic Pyloric Stenosis Tips and Tricks For Ultrasound Diagnosisg1381821Оценок пока нет
- AIUM Practice GuidelineДокумент12 страницAIUM Practice Guidelineg1381821Оценок пока нет
- AppendixДокумент5 страницAppendixg1381821Оценок пока нет
- Sonographic Mimics of Renal CalculiДокумент7 страницSonographic Mimics of Renal Calculig1381821Оценок пока нет
- Ajr 11 6559Документ4 страницыAjr 11 6559g1381821Оценок пока нет
- Introduction To CT TheoryДокумент14 страницIntroduction To CT TheoryManoj100% (2)
- Ielts TASK 1 ExerciseДокумент3 страницыIelts TASK 1 Exerciseanitha nathenОценок пока нет
- ITCC in Riyadh Residential Complex J10-13300 16715-1 Voice & Data Communication CablingДокумент16 страницITCC in Riyadh Residential Complex J10-13300 16715-1 Voice & Data Communication CablinguddinnadeemОценок пока нет
- Comparatives and SuperlativesДокумент2 страницыComparatives and Superlativesjcarlosgf60% (5)
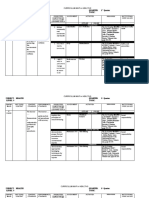
- The Learner The Learner : 1 QuarterДокумент4 страницыThe Learner The Learner : 1 QuarterRode Jane SumambanОценок пока нет
- Research News: Sedimentation Velocity of Solids in Finite Size VesselsДокумент4 страницыResearch News: Sedimentation Velocity of Solids in Finite Size VesselskorangaprakashОценок пока нет
- Basic HomeopathyДокумент2 страницыBasic Homeopathypravin216Оценок пока нет
- Conditional Type 0Документ16 страницConditional Type 0marore100% (1)
- Passive In-Line Chlorination For Drinking Water DiДокумент18 страницPassive In-Line Chlorination For Drinking Water DitefovОценок пока нет
- Chapter1-The Clinical LabДокумент24 страницыChapter1-The Clinical LabNawra AhmadОценок пока нет
- 1896 - Pearson - Mathematical Contributions To The Theory of Evolution. III. Regression, Heredity, and PanmixiaДокумент67 страниц1896 - Pearson - Mathematical Contributions To The Theory of Evolution. III. Regression, Heredity, and PanmixiaNilotpal N SvetlanaОценок пока нет
- Cell Reproduction Practice ExamДокумент5 страницCell Reproduction Practice Examjacky qianОценок пока нет
- Employement ExchangeДокумент22 страницыEmployement ExchangeNeelam ThakurОценок пока нет
- Transmission Line BOQ VIMPДокумент72 страницыTransmission Line BOQ VIMPkajale_shrikant2325Оценок пока нет
- Open Delta Purpose in EFДокумент2 страницыOpen Delta Purpose in EFnmanikandanОценок пока нет
- Scaffolding-Fixed and Mobile: Safety Operating ProceduresДокумент1 страницаScaffolding-Fixed and Mobile: Safety Operating Proceduresmohammed muzammilОценок пока нет
- Soc5352 1331Документ4 страницыSoc5352 1331ChinОценок пока нет
- Cessna 206 Chapter 24 Illustrated Parts CatalogueДокумент33 страницыCessna 206 Chapter 24 Illustrated Parts Cataloguekanwar100% (1)
- 65 70Документ6 страниц65 70kang soon cheolОценок пока нет
- EO MNC 10 June 2022Документ4 страницыEO MNC 10 June 2022LeulaDianneCantosОценок пока нет
- CFM56 3Документ148 страницCFM56 3manmohan100% (1)
- The Safe Motherhood InitiativeДокумент3 страницыThe Safe Motherhood InitiativeAnonymous g6L7jJWОценок пока нет
- Hindustan Coca-Cola Beverages PVT LTD B-91 Mayapuri Industrial Area Phase-I New DelhiДокумент2 страницыHindustan Coca-Cola Beverages PVT LTD B-91 Mayapuri Industrial Area Phase-I New DelhiUtkarsh KadamОценок пока нет
- Ink Presentation Final (TOYO)Документ34 страницыInk Presentation Final (TOYO)komal100% (1)
- BPT Notes Applied PsychologyДокумент36 страницBPT Notes Applied PsychologyVivek Chandra0% (1)
- 138 Student Living: New Returning Yes NoДокумент2 страницы138 Student Living: New Returning Yes NojevaireОценок пока нет
- 004 Torillo v. LeogardoДокумент2 страницы004 Torillo v. LeogardoylessinОценок пока нет
- College RecipesДокумент29 страницCollege RecipeskrunziОценок пока нет
- Personal Loan For JoiningДокумент3 страницыPersonal Loan For JoiningAzim SengalОценок пока нет