Вам также может понравиться
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Doh Health ProgramsДокумент21 страницаDoh Health Programsrgng_1880304050% (2)
- Manual of Clinical Nutrition2013Документ458 страницManual of Clinical Nutrition2013Jeffrey Wheeler100% (9)
- Advances in Nutraceuticals and Functional Foods Concepts and Applications (Gopi Sreerag, Preetha Balakrishnan)Документ378 страницAdvances in Nutraceuticals and Functional Foods Concepts and Applications (Gopi Sreerag, Preetha Balakrishnan)Tanya StepanovaОценок пока нет
- Vegetarian Diets For Children - UpToDateДокумент25 страницVegetarian Diets For Children - UpToDateMaría Paula BelalcazarОценок пока нет
- Format C Programs/Programs/Activities: I. Program On IycfДокумент12 страницFormat C Programs/Programs/Activities: I. Program On IycfKrisna Criselda SimbreОценок пока нет
- Code of General Ordinances of Balete, AklanДокумент31 страницаCode of General Ordinances of Balete, AklanAl F. Dela Cruz100% (3)
- The Ultimate Guide To Dietary SupplementsДокумент18 страницThe Ultimate Guide To Dietary SupplementsNina VodaОценок пока нет
- State Food Provisioning As Social ProtectionДокумент80 страницState Food Provisioning As Social ProtectionJeffrey MarzilliОценок пока нет
- Gender Equality and Food Security: Women's Empowerment As A Tool Against HungerДокумент114 страницGender Equality and Food Security: Women's Empowerment As A Tool Against HungerJeffrey MarzilliОценок пока нет
- Assessment of Potential WFP G2P Partner Programs in IndonesiaДокумент34 страницыAssessment of Potential WFP G2P Partner Programs in IndonesiaJeffrey MarzilliОценок пока нет
- ACAPS Briefing Note Myanmar Floods 6 Aug 2015Документ6 страницACAPS Briefing Note Myanmar Floods 6 Aug 2015Jeffrey MarzilliОценок пока нет
- MIMU Hazard Map Mandalay-Magway Flood Area No. 3 29 Jul 2015Документ1 страницаMIMU Hazard Map Mandalay-Magway Flood Area No. 3 29 Jul 2015Jeffrey MarzilliОценок пока нет
- OCHA Myanmar: Myanmar Rainfall and River Level Forecast OCHA 04 Aug 2015Документ1 страницаOCHA Myanmar: Myanmar Rainfall and River Level Forecast OCHA 04 Aug 2015Jeffrey MarzilliОценок пока нет
- ACAPS Report Southeast Asia Rohingya 07 Aug 2015Документ9 страницACAPS Report Southeast Asia Rohingya 07 Aug 2015Jeffrey MarzilliОценок пока нет
- FES Country Gender Profile - MYANMARДокумент18 страницFES Country Gender Profile - MYANMARJeffrey MarzilliОценок пока нет
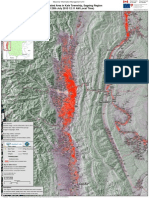
- Myanmar Flood Inundated Area in Kale Townships Sagaing Region 29 Jul 2015Документ1 страницаMyanmar Flood Inundated Area in Kale Townships Sagaing Region 29 Jul 2015Jeffrey MarzilliОценок пока нет
- Hazard Map Myebon Kyaukphyu Ramrees Flood Area 03 Aug 2015 JPJXДокумент1 страницаHazard Map Myebon Kyaukphyu Ramrees Flood Area 03 Aug 2015 JPJXJeffrey MarzilliОценок пока нет
- WFP Myanmar External SitRep Flood Emergency Response 3 Aug 15Документ2 страницыWFP Myanmar External SitRep Flood Emergency Response 3 Aug 15Jeffrey MarzilliОценок пока нет
- WFP Uganda and Burkina Faso's Trial To Reduce Post-Harvest Losses For Smallholder FarmersДокумент4 страницыWFP Uganda and Burkina Faso's Trial To Reduce Post-Harvest Losses For Smallholder FarmersJeffrey MarzilliОценок пока нет
- Myanmar Flood Inundated Area in Kale Townships Sagaing Region 29 Jul 2015Документ1 страницаMyanmar Flood Inundated Area in Kale Townships Sagaing Region 29 Jul 2015Jeffrey MarzilliОценок пока нет
- Key Lessons From The Agriculture Response To Severe Tropical Cyclone PamДокумент9 страницKey Lessons From The Agriculture Response To Severe Tropical Cyclone PamJeffrey MarzilliОценок пока нет
- Philippines Dept of Agriculture Preliminary Estimates of Losses From Typhoon Haiyan (Yolanda) Nov 27, 2013Документ12 страницPhilippines Dept of Agriculture Preliminary Estimates of Losses From Typhoon Haiyan (Yolanda) Nov 27, 2013Jeffrey MarzilliОценок пока нет
- Myanmar Flood Inundated Area in Kale Townships Sagaing Region 29 Jul 2015Документ1 страницаMyanmar Flood Inundated Area in Kale Townships Sagaing Region 29 Jul 2015Jeffrey MarzilliОценок пока нет
- UN SWAP Technical Notes Dec 2013Документ69 страницUN SWAP Technical Notes Dec 2013Jeffrey MarzilliОценок пока нет
- Why Gender?Документ5 страницWhy Gender?Jeffrey MarzilliОценок пока нет
- Vanuatu Tropical Cyclone Pam Situation Report #5 23 Mar 2015Документ2 страницыVanuatu Tropical Cyclone Pam Situation Report #5 23 Mar 2015Jeffrey MarzilliОценок пока нет
- Panay Island Rapid Market Assessment Report, World Vision, Nov 29, 2013Документ16 страницPanay Island Rapid Market Assessment Report, World Vision, Nov 29, 2013Jeffrey MarzilliОценок пока нет
- WFP 2012 Update of Safety Nets Policy - The Role of Food Assistance in Social ProtectionДокумент29 страницWFP 2012 Update of Safety Nets Policy - The Role of Food Assistance in Social ProtectionJeffrey Marzilli100% (1)
- IFRC Strategic Framework On Gender and Diversity 2013-2020Документ8 страницIFRC Strategic Framework On Gender and Diversity 2013-2020Jeffrey MarzilliОценок пока нет
- WFP Kenya's Transitional Cash Transfers To Schools (TCTS) : A Cash-Based Home Grown School Meals ProgrammeДокумент4 страницыWFP Kenya's Transitional Cash Transfers To Schools (TCTS) : A Cash-Based Home Grown School Meals ProgrammeJeffrey MarzilliОценок пока нет
- Panay Island Rapid Market Assessment Report, World Vision, Nov 29, 2013Документ16 страницPanay Island Rapid Market Assessment Report, World Vision, Nov 29, 2013Jeffrey MarzilliОценок пока нет
- Typhoon Haiyan Damage Summary Manila Philippines, Global Agriculture Information Netowrk (GAIN), USDA/FAS, Dec 4, 2013Документ3 страницыTyphoon Haiyan Damage Summary Manila Philippines, Global Agriculture Information Netowrk (GAIN), USDA/FAS, Dec 4, 2013Jeffrey MarzilliОценок пока нет
- WFP Nutrition Policy 2012Документ23 страницыWFP Nutrition Policy 2012Jeffrey MarzilliОценок пока нет
- UNHCR 2009 Policy On Refugee Protection and Solutions in Urban AreasДокумент30 страницUNHCR 2009 Policy On Refugee Protection and Solutions in Urban AreasJeffrey MarzilliОценок пока нет
- Nutrition Recommendations in Pregnancy and LactationДокумент17 страницNutrition Recommendations in Pregnancy and LactationDodi TambunОценок пока нет
- Ferric Sodium Edta (Fena-Edta) : and Its Long and Winding Road Towards Implementation As A Food FortificantДокумент1 страницаFerric Sodium Edta (Fena-Edta) : and Its Long and Winding Road Towards Implementation As A Food Fortificantikhsan07Оценок пока нет
- 5 XerophtalmiaДокумент36 страниц5 XerophtalmiaMarshet GeteОценок пока нет
- Lipofer Technical Report by LipofoodsДокумент16 страницLipofer Technical Report by LipofoodsFernando HuaytaОценок пока нет
- The Heart of The MatterДокумент3 страницыThe Heart of The Mattercklcat1437Оценок пока нет
- CHN (08-31-2021)Документ10 страницCHN (08-31-2021)Enrico LavariasОценок пока нет
- Standards & Quality Control Manual for Edible Salt ManufacturingДокумент46 страницStandards & Quality Control Manual for Edible Salt ManufacturingRana NaveedОценок пока нет
- Food Fortification ProgramДокумент5 страницFood Fortification ProgramChar PereaОценок пока нет
- India's Massive Food Fortification Programme - Conflict of Interest - 2Документ28 страницIndia's Massive Food Fortification Programme - Conflict of Interest - 2maheshmuralinair6Оценок пока нет
- RENI - Guidance Converting Units of Measure For Folate Niacin Vitamins A D E On Nutrition Facts LabelsДокумент31 страницаRENI - Guidance Converting Units of Measure For Folate Niacin Vitamins A D E On Nutrition Facts LabelsSixОценок пока нет
- Nutritional Deficiency AnemiaДокумент6 страницNutritional Deficiency AnemiaShaimaa EmadОценок пока нет
- MAPEH Reviewer for 2nd QuarterДокумент7 страницMAPEH Reviewer for 2nd QuarterGan Josef BoocОценок пока нет
- Vitamins: Vitamin What It Does Where Is It Found Daily Value BiotinДокумент6 страницVitamins: Vitamin What It Does Where Is It Found Daily Value BiotinissaiahnicolleОценок пока нет
- Modern Food Processing - December 2011Документ57 страницModern Food Processing - December 2011infoshareacplОценок пока нет
- SCRAPBOOKДокумент18 страницSCRAPBOOKKervy Jay AgraviadorОценок пока нет
- MERGEFДокумент383 страницыMERGEFmadison DeliОценок пока нет
- Snacks For Children: Targeting A New Generation of Parents: April 2020Документ38 страницSnacks For Children: Targeting A New Generation of Parents: April 2020Nairit MondalОценок пока нет
- Flour FortificationДокумент21 страницаFlour FortificationMarcus WesОценок пока нет
- Honoring God's Creation - Christianity and VegetarianismДокумент16 страницHonoring God's Creation - Christianity and VegetarianismVegan FutureОценок пока нет
- 02 Materi Presentasi Adhi S LukmanДокумент32 страницы02 Materi Presentasi Adhi S LukmanIcoy Pebrina CiciliaОценок пока нет
- National Nutrition ProgrammeДокумент37 страницNational Nutrition ProgrammeEli Zza KoiralaОценок пока нет
- Nutrition Concepts and Controversies 13Th Edition Sizer Solutions Manual Full Chapter PDFДокумент46 страницNutrition Concepts and Controversies 13Th Edition Sizer Solutions Manual Full Chapter PDFinlawbast.ileir100% (8)
- Exam 1 NotesДокумент46 страницExam 1 NotesLes MarОценок пока нет