Вам также может понравиться
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Va41 4 507Документ19 страницVa41 4 507bdalcin5512Оценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5795)
- Va41 4 493Документ14 страницVa41 4 493bdalcin5512Оценок пока нет
- Va41 3 405Документ6 страницVa41 3 405bdalcin5512Оценок пока нет
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Wittgenstein, Semantics and Connectionism: Laurence Goldstein and Hartley Slater, University of Hong KongДокумент22 страницыWittgenstein, Semantics and Connectionism: Laurence Goldstein and Hartley Slater, University of Hong Kongbdalcin5512Оценок пока нет
- Ii. The Investigation: Dendrochronological Dating of Bronze Age Oak CoffinsДокумент4 страницыIi. The Investigation: Dendrochronological Dating of Bronze Age Oak Coffinsbdalcin5512Оценок пока нет
- The Dendrochronological InvestigationДокумент2 страницыThe Dendrochronological Investigationbdalcin5512Оценок пока нет
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Society: V. "Embalming"Документ12 страницSociety: V. "Embalming"bdalcin5512Оценок пока нет
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Vi. Crossdating: Theoretical ConsiderationsДокумент3 страницыVi. Crossdating: Theoretical Considerationsbdalcin5512Оценок пока нет
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- B. Calendars: UnitsДокумент11 страницB. Calendars: Unitsbdalcin5512Оценок пока нет
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Viii. Metal Deposits: Written SourcesДокумент14 страницViii. Metal Deposits: Written Sourcesbdalcin5512Оценок пока нет
- Chronology: La Cronologia È L'occhio Dell'istoriaДокумент3 страницыChronology: La Cronologia È L'occhio Dell'istoriabdalcin5512Оценок пока нет
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- Cosmology: Ix. Lure of The SunДокумент3 страницыCosmology: Ix. Lure of The Sunbdalcin5512Оценок пока нет
- Ii. Dates & "Historical Events": Acta ArchaeologicaДокумент2 страницыIi. Dates & "Historical Events": Acta Archaeologicabdalcin5512Оценок пока нет
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Not PrecedentialДокумент5 страницNot PrecedentialScribd Government DocsОценок пока нет
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Wulandari - Solihin (2016)Документ8 страницWulandari - Solihin (2016)kelvinprd9Оценок пока нет
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Compulsory CounterclaimДокумент4 страницыCompulsory CounterclaimAlexandria FernandoОценок пока нет
- Sanskrit LessonsДокумент195 страницSanskrit LessonsSuganya100% (1)
- ATHE Level 3 Diploma in Business (RQF / 60 Credits)Документ4 страницыATHE Level 3 Diploma in Business (RQF / 60 Credits)GibsonОценок пока нет
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Dnyanadeep's IAS: UPSC Essay Series - 7Документ2 страницыDnyanadeep's IAS: UPSC Essay Series - 7Rahul SinghОценок пока нет
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Aqeedah TahawiyyahДокумент151 страницаAqeedah Tahawiyyahguyii86100% (1)
- ABS Parametric RollДокумент2 страницыABS Parametric RollAdvan Zuidplas100% (1)
- HRM848 Training Techniques and Practices Summer 2021Документ39 страницHRM848 Training Techniques and Practices Summer 2021Dhruvi RajОценок пока нет
- Ujt and PutДокумент35 страницUjt and Putisraeljumbo100% (1)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Whats New PDFДокумент74 страницыWhats New PDFDe Raghu Veer KОценок пока нет
- Bible Study OutlineДокумент2 страницыBible Study OutlineAnonymous v4SN2iMOyОценок пока нет
- CIR v. San Roque Power Corp., G.R. No. 187485, February 12, 2013Документ8 страницCIR v. San Roque Power Corp., G.R. No. 187485, February 12, 2013samaral bentesinkoОценок пока нет
- Chapter02 AnglesДокумент40 страницChapter02 Angleslen16328100% (1)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Heat Transfer OperationsДокумент10 страницHeat Transfer OperationsShafique AhmedОценок пока нет
- Att.3 Training Evaluation For Course Trainer & FacilitiesДокумент2 страницыAtt.3 Training Evaluation For Course Trainer & FacilitiesYusufОценок пока нет
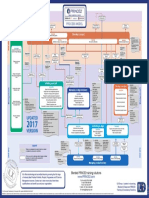
- p2 Process Model 2017Документ1 страницаp2 Process Model 2017Miguel Fernandes0% (1)
- New-Product Development and Product Life-Cycle Strategies GENERAL CONTENT: Multiple-Choice QuestionsДокумент21 страницаNew-Product Development and Product Life-Cycle Strategies GENERAL CONTENT: Multiple-Choice Questionslisa voОценок пока нет
- Kalki ProjectДокумент3 страницыKalki ProjectMandar SohoniОценок пока нет
- "Article Critique" Walden University Methods For Evidence-Based Practice, Nursing 8200 January 28, 2019Документ5 страниц"Article Critique" Walden University Methods For Evidence-Based Practice, Nursing 8200 January 28, 2019Elonna AnneОценок пока нет
- Figures of Speech StylisticsДокумент11 страницFigures of Speech StylisticsCarmie Lactaotao DasallaОценок пока нет
- Academic Calendar 2019-20 Odd Semester PDFДокумент1 страницаAcademic Calendar 2019-20 Odd Semester PDFPiyush ManwaniОценок пока нет
- Engineering ConsultancyДокумент30 страницEngineering Consultancynaconnet100% (2)
- Brief Orientation To Counseling 1st Edition Neukrug Test BankДокумент25 страницBrief Orientation To Counseling 1st Edition Neukrug Test BankStevenAdkinsyjmd100% (55)
- RBG - CRM BRD - Marketing - v4.1Документ68 страницRBG - CRM BRD - Marketing - v4.1Manvi Pareek100% (2)
- Smith Vs CaДокумент11 страницSmith Vs CaIrene QuimsonОценок пока нет
- Fairy Rebel PDFДокумент2 страницыFairy Rebel PDFSamuel0% (1)
- Trust Is The Coin of The Realm by George P. ShultzДокумент13 страницTrust Is The Coin of The Realm by George P. ShultzHoover Institution100% (2)
- News StoryДокумент1 страницаNews StoryRic Anthony LayasanОценок пока нет
- TransModeler BrochureДокумент12 страницTransModeler BrochureedgarabrahamОценок пока нет
- The Age of Magical Overthinking: Notes on Modern IrrationalityОт EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityРейтинг: 4 из 5 звезд4/5 (32)