Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (894)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Parthasarathy2013 PDFДокумент7 страницParthasarathy2013 PDFAndi BintangОценок пока нет
- 1 s2.0 S0002937803001388 MainДокумент3 страницы1 s2.0 S0002937803001388 MainAndi BintangОценок пока нет
- Medical Hypotheses: Yixian Li, Juan Zhou, Ian Burkovskiy, Pollen Yeung, Christian Lehmann TДокумент3 страницыMedical Hypotheses: Yixian Li, Juan Zhou, Ian Burkovskiy, Pollen Yeung, Christian Lehmann TAndi BintangОценок пока нет
- Subarachnoid Block For Caesarean Section in Severe PreeclampsiaДокумент6 страницSubarachnoid Block For Caesarean Section in Severe PreeclampsiaAndi BintangОценок пока нет
- 1 s2.0 S0002937803001388 MainДокумент3 страницы1 s2.0 S0002937803001388 MainAndi BintangОценок пока нет
- Depresión e InmunidadДокумент13 страницDepresión e InmunidadgabisaenaОценок пока нет
- Bar A Zanchi 2018Документ17 страницBar A Zanchi 2018Andi BintangОценок пока нет
- Anestesia General para Césarea PDFДокумент7 страницAnestesia General para Césarea PDFAgnese ValentiniОценок пока нет
- Anestesia General para Césarea PDFДокумент7 страницAnestesia General para Césarea PDFAgnese ValentiniОценок пока нет
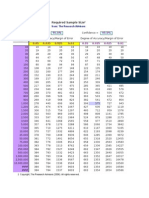
- Required Sample Size: From: The Research AdvisorsДокумент3 страницыRequired Sample Size: From: The Research AdvisorsAbhishek Sharma100% (1)
- Procalcitonin As A Biomarker of Severity Degree in Sepsis Due To PneumoniaДокумент5 страницProcalcitonin As A Biomarker of Severity Degree in Sepsis Due To PneumoniaAndi BintangОценок пока нет
- 1 s2.0 S0002937800704534 Main PDFДокумент1 страница1 s2.0 S0002937800704534 Main PDFAndi BintangОценок пока нет
- Cultural Sociology of Mental Illness n28Документ5 страницCultural Sociology of Mental Illness n28Andi BintangОценок пока нет
- Overweight linked to increased risk of lower back painДокумент8 страницOverweight linked to increased risk of lower back painAndi BintangОценок пока нет
- Instruction For Author ClimactericДокумент9 страницInstruction For Author ClimactericAndi BintangОценок пока нет
- 1 s2.0 S1052305714000561 MainДокумент6 страниц1 s2.0 S1052305714000561 MainAndi BintangОценок пока нет
- Hepatitis C APASLfghДокумент27 страницHepatitis C APASLfghAndi BintangОценок пока нет
- Sacral Nerve Stimulation Reduces Elevated Urinary Nerve Growth Factor Levels in Women With Symptomatic Detrusor OveractivityДокумент5 страницSacral Nerve Stimulation Reduces Elevated Urinary Nerve Growth Factor Levels in Women With Symptomatic Detrusor OveractivityAndi BintangОценок пока нет
- 1 s2.0 S0021755713002003 MainДокумент6 страниц1 s2.0 S0021755713002003 MainAndi BintangОценок пока нет
- 1 s2.0 S0021755713002003 MainДокумент6 страниц1 s2.0 S0021755713002003 MainAndi BintangОценок пока нет
- Association Between Constipation and Colorectal Cancer Systematic Review and Meta-Analysis of Observational StusdgdiesДокумент10 страницAssociation Between Constipation and Colorectal Cancer Systematic Review and Meta-Analysis of Observational StusdgdiesAndi BintangОценок пока нет
- 2013 Student Membership ApplicationДокумент1 страница2013 Student Membership ApplicationAndi BintangОценок пока нет
- Prevalence of Diabetes and Impaired Fasting Glucose in Adults in The U.S. PopulationДокумент6 страницPrevalence of Diabetes and Impaired Fasting Glucose in Adults in The U.S. PopulationAndi BintangОценок пока нет
- Anthropometry: Ergonomics Additional ResourcesДокумент5 страницAnthropometry: Ergonomics Additional ResourcesAndi BintangОценок пока нет
- Serviks DocjhjuДокумент366 страницServiks DocjhjuAndi BintangОценок пока нет
- Urologi PDFДокумент237 страницUrologi PDFAndi BintangОценок пока нет
- MK Giz Slide Infant Feeding PracticeДокумент1 страницаMK Giz Slide Infant Feeding PracticeAndi BintangОценок пока нет
- ATS Guidelines CAP ManagementДокумент25 страницATS Guidelines CAP ManagementMae Matira AbeladorОценок пока нет
- PCT CAP ABiuytoДокумент10 страницPCT CAP ABiuytoAndi BintangОценок пока нет
- Cap Bts 2009 ComplitdgДокумент139 страницCap Bts 2009 ComplitdgAndi BintangОценок пока нет
- Rajiv Gandhi University of Health Sciences, Bangalore, Karnataka Synopsis Proforma For Registration of Subjects For DissertationДокумент14 страницRajiv Gandhi University of Health Sciences, Bangalore, Karnataka Synopsis Proforma For Registration of Subjects For Dissertationpavin0% (1)
- Chapter 10 Microbial Ecology and Microbial BiotechnologyДокумент6 страницChapter 10 Microbial Ecology and Microbial BiotechnologyChristel CabanalОценок пока нет
- Signs and SymptomsДокумент6 страницSigns and Symptomsdareine22Оценок пока нет
- Horn Fly and Stable FlyДокумент39 страницHorn Fly and Stable Flylady ann jimenezОценок пока нет
- SOP Air Ambulance-IsakovДокумент6 страницSOP Air Ambulance-IsakovSankar CdmОценок пока нет
- NCP Infective Airway ClearanceДокумент4 страницыNCP Infective Airway ClearanceCherrie Mae PadernaОценок пока нет
- Journal of Feline Medicine and Surgery 2013 Scherk 785 808Документ26 страницJournal of Feline Medicine and Surgery 2013 Scherk 785 808Roberto RibeiroОценок пока нет
- Utbk Level 4Документ4 страницыUtbk Level 4Charisa MarthaОценок пока нет
- Dengvaxia 1. Goals in Relation To The Company's Mission StatementДокумент13 страницDengvaxia 1. Goals in Relation To The Company's Mission StatementShannen Dela CruzОценок пока нет
- 5 Benign Febrile Convulsions Nursing Care PlansДокумент19 страниц5 Benign Febrile Convulsions Nursing Care Plansaaron tabernaОценок пока нет
- Food Quality, Food-Borne Diseases, and Food Safety in The Brazilian Food IndustryДокумент15 страницFood Quality, Food-Borne Diseases, and Food Safety in The Brazilian Food IndustryAnil BhattiОценок пока нет
- Arachnids of Medical Importance (Ticks and MitesДокумент26 страницArachnids of Medical Importance (Ticks and MitesCLEMENT100% (1)
- Case Study Portfolio - MorehouseДокумент22 страницыCase Study Portfolio - Morehouseapi-347779459Оценок пока нет
- Visiting Scholar ChecklistДокумент9 страницVisiting Scholar Checklistসোমনাথ মহাপাত্রОценок пока нет
- Ecologia de Enfermedades Infecciosas EmergentesДокумент14 страницEcologia de Enfermedades Infecciosas EmergentesJONATHAN DAVID SANCHEZ RODRIGUEZОценок пока нет
- "Community Pest": NSTP 2 Worksheet 6 Project Implementation PlanДокумент2 страницы"Community Pest": NSTP 2 Worksheet 6 Project Implementation PlanRalph B. BarsanalinaОценок пока нет
- Trypanosomiasis in CamelsДокумент20 страницTrypanosomiasis in CamelsAnugat Jena0% (1)
- Coccidioidomycosis A Contemporary ReviewДокумент30 страницCoccidioidomycosis A Contemporary ReviewMIGUELОценок пока нет
- IN - AJA - Dazel Kit - Plan - V1 - 19042016Документ16 страницIN - AJA - Dazel Kit - Plan - V1 - 19042016nagaraj2675Оценок пока нет
- Guidelines in BedmakingДокумент9 страницGuidelines in Bedmakinglex aspira100% (1)
- Fusidic Acid in Dermatology: An Updated ReviewДокумент10 страницFusidic Acid in Dermatology: An Updated ReviewKevin FloresОценок пока нет
- MYCOДокумент59 страницMYCOAngela ReyesОценок пока нет
- BrucellosisДокумент55 страницBrucellosistummalapalli venkateswara rao50% (2)
- Tutorial 1Документ3 страницыTutorial 1Keefwat TawfeekОценок пока нет
- Betty Knight's "6F S": FluidsДокумент1 страницаBetty Knight's "6F S": FluidsESTHER OGODOОценок пока нет
- Bettaboxx Betta Illness GuideДокумент13 страницBettaboxx Betta Illness Guiderichard nyeОценок пока нет
- Philippines National Immunization Program Goals and GuidelinesДокумент29 страницPhilippines National Immunization Program Goals and Guidelineselle leliОценок пока нет
- National Antibiotic Guideline 2014 Full VersionДокумент246 страницNational Antibiotic Guideline 2014 Full Versionevonnecheah100% (2)
- Infectious Diarrhea Mechanisms and EtiologyДокумент75 страницInfectious Diarrhea Mechanisms and EtiologyFany Raihan PadilahОценок пока нет
- Gdocs Trans TemplateДокумент3 страницыGdocs Trans TemplateshichiОценок пока нет