Вам также может понравиться
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Cancer AwarenessДокумент20 страницCancer AwarenessArul Nambi Ramanujam100% (3)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- 1 GYNE 2 Emotional Aspects of GynecologyДокумент4 страницы1 GYNE 2 Emotional Aspects of GynecologyIrene FranzОценок пока нет
- 10 Introductory Questions Therapists Commonly Ask PDFДокумент4 страницы10 Introductory Questions Therapists Commonly Ask PDFsamir shah100% (1)
- Steven K. Huprich - Psychodynamic Therapy - Conceptual and Empirical Foundations (2008) PDFДокумент288 страницSteven K. Huprich - Psychodynamic Therapy - Conceptual and Empirical Foundations (2008) PDFChalwe HowardОценок пока нет
- Hypertension CASE STUDYДокумент30 страницHypertension CASE STUDYKaloy Kamao100% (7)
- Dr. Nyoman - Neuropsychiatric Systemic Lupus Erythematosus (NPSLE) .Документ41 страницаDr. Nyoman - Neuropsychiatric Systemic Lupus Erythematosus (NPSLE) .hum2Оценок пока нет
- Sample Psychiatric Case StudyДокумент8 страницSample Psychiatric Case StudyAlphonse Nazario50% (2)
- Guidance ServicesДокумент56 страницGuidance Servicesminna comuyogОценок пока нет
- OralMeds - ChecklistДокумент6 страницOralMeds - ChecklistXandra BasnilloОценок пока нет
- Roots 1 - 2015Документ60 страницRoots 1 - 2015Ovidiu100% (1)
- P ('t':3) Var B Location Settimeout (Function (If (Typeof Window - Iframe 'Undefined') (B.href B.href ) ), 15000)Документ1 страницаP ('t':3) Var B Location Settimeout (Function (If (Typeof Window - Iframe 'Undefined') (B.href B.href ) ), 15000)Milanisti22Оценок пока нет
- Typhoid FeverДокумент6 страницTyphoid FeverReeshabhdev GauttamОценок пока нет
- Trichomonas Vaginalis Vaginitis in Obstetrics and Gynecology Practice - New Concepts and ControversiesДокумент12 страницTrichomonas Vaginalis Vaginitis in Obstetrics and Gynecology Practice - New Concepts and Controversieshimono_onaОценок пока нет
- WisconsinДокумент2 страницыWisconsinhimono_onaОценок пока нет
- (2008) Long-acting β2-agonists (LABA) in chronic obstructive pulmonary disease- efficacy and safetyДокумент10 страниц(2008) Long-acting β2-agonists (LABA) in chronic obstructive pulmonary disease- efficacy and safetyhimono_onaОценок пока нет
- CDM Antibio1 PhagyngitisTonsillitis enДокумент2 страницыCDM Antibio1 PhagyngitisTonsillitis enhimono_onaОценок пока нет
- Serum Zink in SeizureДокумент5 страницSerum Zink in SeizurevinominiОценок пока нет
- Corticosteroid in Copd ExacerbationДокумент6 страницCorticosteroid in Copd Exacerbationhimono_onaОценок пока нет
- Cervical Paravertebral BlockДокумент6 страницCervical Paravertebral Blockhimono_onaОценок пока нет
- Jurnal1 PDFДокумент5 страницJurnal1 PDFhimono_onaОценок пока нет
- Period On Tit IsДокумент7 страницPeriod On Tit Ishimono_onaОценок пока нет
- What Is Alzheimer's - Alzheimer's AssociationДокумент6 страницWhat Is Alzheimer's - Alzheimer's AssociationRatnaPrasadNalamОценок пока нет
- Act For Insomnia Act I by DR Guy Meadows The Sleep SchoolДокумент7 страницAct For Insomnia Act I by DR Guy Meadows The Sleep SchoolDharmendra KumarОценок пока нет
- Pharmacology Table For Cardiovascular LectureДокумент10 страницPharmacology Table For Cardiovascular LecturemuhammadridhwanОценок пока нет
- Sample Size PilotДокумент5 страницSample Size PilotmsriramcaОценок пока нет
- Oxaliplatin Monograph 1dec2016Документ9 страницOxaliplatin Monograph 1dec2016Nadial UzmahОценок пока нет
- Bladder Diverticulum and SepsisДокумент4 страницыBladder Diverticulum and SepsisInternational Medical PublisherОценок пока нет
- Sex ChangeДокумент17 страницSex ChangesoberanoriofionaОценок пока нет
- Tetralogy Hypercyanotic SpellДокумент3 страницыTetralogy Hypercyanotic SpellJunior PratasikОценок пока нет
- Laporan Stok Op Farmasi Smec Center Lembean April 2021Документ65 страницLaporan Stok Op Farmasi Smec Center Lembean April 2021Hafidz MokodompitОценок пока нет
- Katerina P Reilly ResumeДокумент2 страницыKaterina P Reilly Resumeapi-286221742Оценок пока нет
- TM ModuleДокумент57 страницTM Moduleprincess lyn castromayorОценок пока нет
- Challenges in Care of Adult CF Patients - The Specialist Cystic Fibrosis TeamДокумент4 страницыChallenges in Care of Adult CF Patients - The Specialist Cystic Fibrosis TeamjuniorebindaОценок пока нет
- Pre Analytical Clot EdДокумент12 страницPre Analytical Clot EdAnonymous w4qodCJОценок пока нет
- Novartis NVS Q4 2016 Ir PresentationДокумент84 страницыNovartis NVS Q4 2016 Ir PresentationmedtechyОценок пока нет
- What Are The Benefits of An Intensive Outpatient ProgramДокумент2 страницыWhat Are The Benefits of An Intensive Outpatient ProgramDan MarkОценок пока нет
- Lymphoma HandoutДокумент5 страницLymphoma Handoutapi-244850728Оценок пока нет
- Ileocecal ResectionДокумент12 страницIleocecal ResectionPVP BOSNIAОценок пока нет
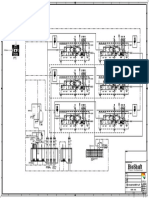
- P&ID - STP-Yanbu SWCC (6units)Документ1 страницаP&ID - STP-Yanbu SWCC (6units)Ashraf BayomiОценок пока нет
- Cholelithiasis & CholecystitisДокумент2 страницыCholelithiasis & CholecystitisKate DОценок пока нет
- Module 4 (Basics of Sti, Hiv & Aids)Документ37 страницModule 4 (Basics of Sti, Hiv & Aids)Marky RoqueОценок пока нет