Вам также может понравиться
- Epilepsy and Newer Drugs.Документ70 страницEpilepsy and Newer Drugs.Ch Rajesh100% (1)
- Understanding Muscle TwitchesДокумент10 страницUnderstanding Muscle TwitchesAndiena ElsafiraОценок пока нет
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (890)
- Mysthenia Gravis DR NajeebДокумент11 страницMysthenia Gravis DR NajeebJay kumarОценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
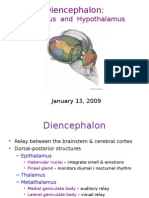
- Thalamus Hypothalamus GajДокумент55 страницThalamus Hypothalamus GajMédecin Adrian TGОценок пока нет
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- Past Papers FCPS NeurologyДокумент10 страницPast Papers FCPS NeurologyZaid WaqarОценок пока нет
- Diagnose and manage IAN injuryДокумент7 страницDiagnose and manage IAN injuryNeil SchembriОценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- (G1) What Triggers ADHDДокумент24 страницы(G1) What Triggers ADHDhvtvan0702Оценок пока нет
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Drugs For Parkinson's Disease: Pharmacist'S Letter / Prescriber'S LetterДокумент4 страницыDrugs For Parkinson's Disease: Pharmacist'S Letter / Prescriber'S Letteranon_84599888Оценок пока нет
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Writer's Cramp - WikipediaДокумент17 страницWriter's Cramp - WikipediaMihailoОценок пока нет
- Sem-3 Physiology of PainДокумент69 страницSem-3 Physiology of PainJyoti Pol SherkhaneОценок пока нет
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Neurology EMQДокумент5 страницNeurology EMQLakshya J BasumataryОценок пока нет
- IV. Modul 10 - Pengelolaan NyeriДокумент97 страницIV. Modul 10 - Pengelolaan NyeriGrace Noviyanthi SinambelaОценок пока нет
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Meniere's Disease: Leona Šupljika GabelicaДокумент17 страницMeniere's Disease: Leona Šupljika GabelicaAlvarendra RationoОценок пока нет
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Current Views On Treatment of Vertigo and Dizziness (JURDING)Документ22 страницыCurrent Views On Treatment of Vertigo and Dizziness (JURDING)arifОценок пока нет
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- Anatomy and Physiology of NeuronsДокумент4 страницыAnatomy and Physiology of NeuronsVan Jasper Pimentel BautistaОценок пока нет
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Mudra For Nervous System Disorders (Video) - Complete PersonДокумент5 страницMudra For Nervous System Disorders (Video) - Complete PersonArun KumarОценок пока нет
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Risk of Sound-Induced Hearing Disorders For Audio Post Production Engineers: A Preliminary StudyДокумент10 страницRisk of Sound-Induced Hearing Disorders For Audio Post Production Engineers: A Preliminary StudylauraОценок пока нет
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- Thomas D. Parsons (Auth.) - Clinical Neuropsychology and Technology - What's New and How We Can Use It (2016, Springer International Publishing)Документ198 страницThomas D. Parsons (Auth.) - Clinical Neuropsychology and Technology - What's New and How We Can Use It (2016, Springer International Publishing)Ever Josue Alvarenga100% (2)
- Edition: You Are Logged-InДокумент142 страницыEdition: You Are Logged-InJoenabie Andoy Encanto0% (1)
- Essential Perimetry The Field Analyzer PrimerДокумент162 страницыEssential Perimetry The Field Analyzer PrimerDavid Croes100% (1)
- The Compass 2015Документ178 страницThe Compass 2015Venture PublishingОценок пока нет
- Reflex Testing Methods For Evaluating CNS DevelopmentДокумент80 страницReflex Testing Methods For Evaluating CNS DevelopmentTaufik100% (4)
- Nervous TissueДокумент7 страницNervous TissueDavid CalaloОценок пока нет
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Epilepsy and Seizure Assessment and Management GuideTITLEДокумент31 страницаEpilepsy and Seizure Assessment and Management GuideTITLEKyle Ü D. CunanersОценок пока нет
- Scoring PSGДокумент23 страницыScoring PSGMilky UniqueОценок пока нет
- Diagnosis and Initial Treatment of Ischemic Stroke: Health Care GuidelineДокумент71 страницаDiagnosis and Initial Treatment of Ischemic Stroke: Health Care GuidelineRosyid PrasetyoОценок пока нет
- Central Positional VertigoДокумент428 страницCentral Positional Vertigoveerraju tvОценок пока нет
- DAFTAR PASIEN BEDAH SARAF 11 JANUARI 2022Документ2 страницыDAFTAR PASIEN BEDAH SARAF 11 JANUARI 2022bobirfansyahputraОценок пока нет
- AphasiaДокумент208 страницAphasiaErika Velásquez100% (4)
- Case Report NeurologyДокумент2 страницыCase Report NeurologyMuhammad ArifinОценок пока нет
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)