Вам также может понравиться
- Quarantine Label - LT3!13!03Документ1 страницаQuarantine Label - LT3!13!03William ChandraОценок пока нет
- English Text Label, Thailand, 3 ML, (LT3) : Retention SampleДокумент1 страницаEnglish Text Label, Thailand, 3 ML, (LT3) : Retention SampleWilliam ChandraОценок пока нет
- Quarantine Label - LT3!13!02Документ1 страницаQuarantine Label - LT3!13!02William ChandraОценок пока нет
- Approved Label - LT3!12!02Документ1 страницаApproved Label - LT3!12!02William ChandraОценок пока нет
- English Text Label, Thailand, 3 ML, (LT3) : Retention SampleДокумент1 страницаEnglish Text Label, Thailand, 3 ML, (LT3) : Retention SampleWilliam ChandraОценок пока нет
- Borden Co. (Pte.) LTD.: Starting Materials Record (Status After Testing)Документ2 страницыBorden Co. (Pte.) LTD.: Starting Materials Record (Status After Testing)William ChandraОценок пока нет
- English Text Label, Thailand, 6 ML, (LT2) : Retention SampleДокумент1 страницаEnglish Text Label, Thailand, 6 ML, (LT2) : Retention SampleWilliam ChandraОценок пока нет
- English Text Label, Thailand, 6 ML, (LT2) : Retention SampleДокумент1 страницаEnglish Text Label, Thailand, 6 ML, (LT2) : Retention SampleWilliam ChandraОценок пока нет
- QC Approved QC Approved QC Approved: 15 PiecesДокумент1 страницаQC Approved QC Approved QC Approved: 15 PiecesWilliam ChandraОценок пока нет
- Form SMR.11T.L - LT2-13-03Документ2 страницыForm SMR.11T.L - LT2-13-03William ChandraОценок пока нет
- Approved Label - LT3!12!02Документ1 страницаApproved Label - LT3!12!02William ChandraОценок пока нет
- Borden Co. (Pte.) LTD.: Starting Materials RecordДокумент2 страницыBorden Co. (Pte.) LTD.: Starting Materials RecordWilliam ChandraОценок пока нет
- Quality Control Packaging Materials Receiving RecordДокумент2 страницыQuality Control Packaging Materials Receiving RecordWilliam ChandraОценок пока нет
- QC Approved QC Approved QC Approved: 15 PiecesДокумент1 страницаQC Approved QC Approved QC Approved: 15 PiecesWilliam ChandraОценок пока нет
- Borden Co. (Pte.) LTD.: Starting Materials Record (Status After Testing)Документ2 страницыBorden Co. (Pte.) LTD.: Starting Materials Record (Status After Testing)William ChandraОценок пока нет
- Borden Co. (Pte.) LTD.: Starting Materials Record (Status After Testing)Документ2 страницыBorden Co. (Pte.) LTD.: Starting Materials Record (Status After Testing)William ChandraОценок пока нет
- QC Approved QC Approved QC Approved: 15 PiecesДокумент1 страницаQC Approved QC Approved QC Approved: 15 PiecesWilliam ChandraОценок пока нет
- Borden Co. (Pte.) LTD.: Starting Materials RecordДокумент2 страницыBorden Co. (Pte.) LTD.: Starting Materials RecordWilliam ChandraОценок пока нет
- English Text Label, Thailand, 6 ML, (LT2) : Retention SampleДокумент1 страницаEnglish Text Label, Thailand, 6 ML, (LT2) : Retention SampleWilliam ChandraОценок пока нет
- Quarantine Label - LT3!12!02Документ1 страницаQuarantine Label - LT3!12!02William ChandraОценок пока нет
- Borden Co. (Pte.) LTD.: Starting Materials RecordДокумент2 страницыBorden Co. (Pte.) LTD.: Starting Materials RecordWilliam ChandraОценок пока нет
- QC Approved QC Approved QC Approved: 15 PiecesДокумент1 страницаQC Approved QC Approved QC Approved: 15 PiecesWilliam ChandraОценок пока нет
- QC Approved QC Approved QC Approved: 15 PiecesДокумент1 страницаQC Approved QC Approved QC Approved: 15 PiecesWilliam ChandraОценок пока нет
- Quarantine Label - LT3!12!01Документ1 страницаQuarantine Label - LT3!12!01William ChandraОценок пока нет
- English Text Label, Thailand, 3 ML, (LT3) : Retention SampleДокумент1 страницаEnglish Text Label, Thailand, 3 ML, (LT3) : Retention SampleWilliam ChandraОценок пока нет
- Approved Label - LT3!12!01Документ1 страницаApproved Label - LT3!12!01William ChandraОценок пока нет
- English Text Label, Thailand, 12 ML, (LT1) : Retention SampleДокумент1 страницаEnglish Text Label, Thailand, 12 ML, (LT1) : Retention SampleWilliam ChandraОценок пока нет
- English Text Label, Thailand, 6 ML, (LT2) : Retention SampleДокумент1 страницаEnglish Text Label, Thailand, 6 ML, (LT2) : Retention SampleWilliam ChandraОценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5795)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Calculating Medical DosagesДокумент14 страницCalculating Medical DosagesJennifer Jaworsky100% (3)
- ATSP Booklet 2019 FinalДокумент24 страницыATSP Booklet 2019 FinalShreya BОценок пока нет
- Frozen ShoulderДокумент44 страницыFrozen ShoulderEspers BluesОценок пока нет
- BONEJДокумент3 страницыBONEJZohair AlamОценок пока нет
- The House Tree and Person TestДокумент10 страницThe House Tree and Person TestRidaОценок пока нет
- Happiful June 2022Документ92 страницыHappiful June 2022Лера СавченкоОценок пока нет
- Blume - When Therapists CryДокумент245 страницBlume - When Therapists CryPixie Willo100% (2)
- Exam in MS1 Cope 2nd ExamДокумент5 страницExam in MS1 Cope 2nd ExamIbrahim RegachoОценок пока нет
- Definition of Aquatic ExerciseДокумент3 страницыDefinition of Aquatic Exercisevenkata ramakrishnaiahОценок пока нет
- 04IJPHY907Документ8 страниц04IJPHY907ize browniezОценок пока нет
- Sudarshan Kriya - Sri Sri Ravi Shankar - Interesting - Facts - SKДокумент3 страницыSudarshan Kriya - Sri Sri Ravi Shankar - Interesting - Facts - SKndhantaОценок пока нет
- Nclex PNДокумент416 страницNclex PNSandhu Sdhu100% (9)
- PLAB ENT MCQsДокумент27 страницPLAB ENT MCQsKay Bristol100% (1)
- Ekdahl 2010Документ8 страницEkdahl 2010ika kurniawatiОценок пока нет
- P. PellucidaДокумент32 страницыP. PellucidaMartin OgbacОценок пока нет
- Perioral DermatitisДокумент5 страницPerioral DermatitisAstriana IndrawatiОценок пока нет
- TTSH Nursing Survival GuideДокумент96 страницTTSH Nursing Survival GuideSarip Dol100% (2)
- Kotak Health Premier Claim Form Part BДокумент32 страницыKotak Health Premier Claim Form Part BRKОценок пока нет
- 1246 PDFДокумент4 страницы1246 PDFPrima RiyandiОценок пока нет
- New Problem StatementДокумент2 страницыNew Problem Statementrenuka rathore100% (2)
- Drug Study FormatДокумент2 страницыDrug Study FormatEmilie CajaОценок пока нет
- Towards Improving post-SSRI Sexual Dysfunction by Using Nutriceuticals: Lessons From A Case Study - Calabrò 2019Документ8 страницTowards Improving post-SSRI Sexual Dysfunction by Using Nutriceuticals: Lessons From A Case Study - Calabrò 2019Julio JuarezОценок пока нет
- SyncopeДокумент105 страницSyncopeJohn DasОценок пока нет
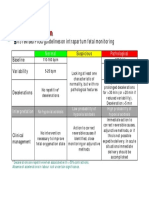
- CTG Classification PDFДокумент1 страницаCTG Classification PDFganotОценок пока нет
- Chapter 07 Treatment PlanningДокумент232 страницыChapter 07 Treatment PlanningAhmed Ridwan OladotunОценок пока нет
- AAA Mixed Pain SMGДокумент37 страницAAA Mixed Pain SMGandhita96Оценок пока нет
- ENTДокумент20 страницENTGaurav BatniОценок пока нет
- DSWD PWDДокумент5 страницDSWD PWDFar GausОценок пока нет
- 2c.4S Framework For Mental HealthДокумент3 страницы2c.4S Framework For Mental HealthByaruhanga EmmanuelОценок пока нет
- Angle Class II, Division 2, Malocclusion With Deep OverbiteДокумент12 страницAngle Class II, Division 2, Malocclusion With Deep OverbiteDianaОценок пока нет