Вам также может понравиться
- Youth Volunteering in Africa The Case of The Au Youth Volunteers CorpsДокумент12 страницYouth Volunteering in Africa The Case of The Au Youth Volunteers CorpsNeo Mervyn MonahengОценок пока нет
- Ce Foundtn Manual Edited PDFДокумент30 страницCe Foundtn Manual Edited PDFNeo Mervyn Monaheng67% (6)
- SKEPP 2011 Nanomaterials - in - REACH - Report - 15082011 PDFДокумент239 страницSKEPP 2011 Nanomaterials - in - REACH - Report - 15082011 PDFNeo Mervyn MonahengОценок пока нет
- Practical Manual Converted Final 2017Документ43 страницыPractical Manual Converted Final 2017Neo Mervyn MonahengОценок пока нет
- Chap2 Power Point PresentationДокумент74 страницыChap2 Power Point PresentationNeo Mervyn MonahengОценок пока нет
- Botha 2 Comparative Aquatic Toxicity of - Gold NanoparticlesДокумент8 страницBotha 2 Comparative Aquatic Toxicity of - Gold NanoparticlesNeo Mervyn MonahengОценок пока нет
- Gulumian SAJS 2012Документ9 страницGulumian SAJS 2012Neo Mervyn MonahengОценок пока нет
- DR McCormick Academic Essay Notes February 2017Документ9 страницDR McCormick Academic Essay Notes February 2017Neo Mervyn MonahengОценок пока нет
- A Review On Nanomaterials For Environmental RemediationДокумент35 страницA Review On Nanomaterials For Environmental RemediationNeo Mervyn MonahengОценок пока нет
- The Blood Covenant: by Mindena SpurlingДокумент33 страницыThe Blood Covenant: by Mindena SpurlingNeo Mervyn MonahengОценок пока нет
- Caps Fet - Life Sciences - GR 10-12 Web - 2636Документ82 страницыCaps Fet - Life Sciences - GR 10-12 Web - 2636Neo Mervyn Monaheng50% (2)
- Mathematics 1 Tutorials 2017Документ66 страницMathematics 1 Tutorials 2017Neo Mervyn MonahengОценок пока нет
- The Citizen - Laboratory Scientist Degree Created - 25 OctoberДокумент1 страницаThe Citizen - Laboratory Scientist Degree Created - 25 OctoberNeo Mervyn MonahengОценок пока нет
- Class 6 Handout 3 Poster GM CropsДокумент1 страницаClass 6 Handout 3 Poster GM CropsNeo Mervyn MonahengОценок пока нет
- Joint and by Products 2016Документ20 страницJoint and by Products 2016Neo Mervyn MonahengОценок пока нет
- CBL ExhibitДокумент1 страницаCBL ExhibitNeo Mervyn MonahengОценок пока нет
- Bachelor of CommerceДокумент1 страницаBachelor of CommerceNeo Mervyn MonahengОценок пока нет
- Class 1 Handout 3 Topics in Nanobtposter Traditional BiotechДокумент1 страницаClass 1 Handout 3 Topics in Nanobtposter Traditional BiotechNeo Mervyn MonahengОценок пока нет
- 9LHДокумент1 страница9LHNeo Mervyn MonahengОценок пока нет
- Acute Promylocytic LeukaemiaДокумент2 страницыAcute Promylocytic LeukaemiaNeo Mervyn Monaheng100% (1)
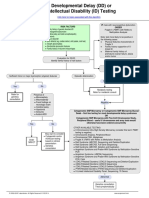
- Developmental Delay (DD) or Intellectual Disability (ID) Testing AlgorithmДокумент1 страницаDevelopmental Delay (DD) or Intellectual Disability (ID) Testing AlgorithmNeo Mervyn Monaheng100% (1)
- Class 1 Handout 2 Topics in Nanobt Poster Biotech TimelineДокумент1 страницаClass 1 Handout 2 Topics in Nanobt Poster Biotech TimelineNeo Mervyn MonahengОценок пока нет
- 2 CytoUserGuide 6.0Документ134 страницы2 CytoUserGuide 6.0Neo Mervyn MonahengОценок пока нет
- 6th Central Pay Commission Salary CalculatorДокумент15 страниц6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- Density Functional TheoryДокумент3 страницыDensity Functional TheoryNeo Mervyn MonahengОценок пока нет
- Ye Are GodsДокумент2 страницыYe Are GodsNeo Mervyn MonahengОценок пока нет
- Dr. Johnson Segment 2 Lecture NotesДокумент3 страницыDr. Johnson Segment 2 Lecture NotesNeo Mervyn MonahengОценок пока нет
- MSc Clinical Epidemiology at Stellenbosch UniversityДокумент24 страницыMSc Clinical Epidemiology at Stellenbosch UniversityNeo Mervyn MonahengОценок пока нет
- (Nicodemus Visits Jesus) : Presented by Sermons 4 Kids Featuring The Art of Henry MartinДокумент10 страниц(Nicodemus Visits Jesus) : Presented by Sermons 4 Kids Featuring The Art of Henry MartinNeo Mervyn MonahengОценок пока нет
- Workflow 2Документ3 страницыWorkflow 2Neo Mervyn MonahengОценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- File PDFДокумент118 страницFile PDFFatemeh BemanaОценок пока нет
- NICE - SSI Prevention and TreatmentДокумент27 страницNICE - SSI Prevention and Treatmentshrinkhala bhattaraiОценок пока нет
- Mrsa SopДокумент3 страницыMrsa Sopajiarosid0Оценок пока нет
- Gram-Negative Bacteria: Antibiogram of Bacteria - Year 2020 (Icu at Kfafh)Документ2 страницыGram-Negative Bacteria: Antibiogram of Bacteria - Year 2020 (Icu at Kfafh)jen nalusОценок пока нет
- Management and Outcome of Sepsis in Term and Late Preterm Infants - UpToDateДокумент21 страницаManagement and Outcome of Sepsis in Term and Late Preterm Infants - UpToDateAlbert SongОценок пока нет
- Maintenance and Preservation of Microbial Cultures PDFДокумент16 страницMaintenance and Preservation of Microbial Cultures PDFyogesh kumarОценок пока нет
- Gram-Positive Cocci Quiz #1Документ9 страницGram-Positive Cocci Quiz #1Stephany Mae ChiОценок пока нет
- 4 - Medicine - MCQs - Infectious DiseaseДокумент7 страниц4 - Medicine - MCQs - Infectious DiseaseAmitОценок пока нет
- Study of The Antibacterial Activities of Soursop (Annona Muricata L.) LeavesДокумент8 страницStudy of The Antibacterial Activities of Soursop (Annona Muricata L.) LeavesAstri Ggamjong Xiao LuОценок пока нет
- Diabetic Foot InfectionДокумент26 страницDiabetic Foot InfectionAmanda Abdat100% (1)
- Malacidine Metagenomic AssayДокумент10 страницMalacidine Metagenomic AssayNCIPDОценок пока нет
- Antiseptics in The Era of Bacterial Resistance A Focus On Povidone IodineДокумент14 страницAntiseptics in The Era of Bacterial Resistance A Focus On Povidone IodinewatidinaОценок пока нет
- Applied Mathematical ModelingДокумент14 страницApplied Mathematical ModelingJaney Hernan MessiasОценок пока нет
- Clinical Bacteriology of Staphylococcus aureusДокумент5 страницClinical Bacteriology of Staphylococcus aureusAnne MorenoОценок пока нет
- Inpatient Treatment of CAP in ChildrenДокумент23 страницыInpatient Treatment of CAP in ChildrenJunny Yeliitza Wilches GualdronОценок пока нет
- Antibiotics - Chua EДокумент29 страницAntibiotics - Chua EerikaОценок пока нет
- International Journal of Recent Scientific ResearchДокумент5 страницInternational Journal of Recent Scientific ResearchifahInayahОценок пока нет
- Burton's Microbiology For The Health Sciences Section V. Environmental and Applied MicrobiologyДокумент32 страницыBurton's Microbiology For The Health Sciences Section V. Environmental and Applied MicrobiologyMitzi Audrey100% (1)
- Clinically Important Pathogenic Bacteria and Their Infectious DiseasesДокумент19 страницClinically Important Pathogenic Bacteria and Their Infectious DiseasesanumОценок пока нет
- Resisten AntibiotikДокумент218 страницResisten AntibiotikYano FiandiОценок пока нет
- Antimicrobial AgentsДокумент34 страницыAntimicrobial Agentssuchi_mohan08Оценок пока нет
- Harrisons Reviewer 2Документ59 страницHarrisons Reviewer 2pluiedecielОценок пока нет
- Acute Cellulitis and Erysipelas in Adults - Treatment - UpToDateДокумент28 страницAcute Cellulitis and Erysipelas in Adults - Treatment - UpToDateYahir PerezОценок пока нет
- Staph and Strep IdentificationДокумент22 страницыStaph and Strep Identificationrazgriz1100% (1)
- 8C1DF0AECDF8E231Документ49 страниц8C1DF0AECDF8E231Jmarc JubiladoОценок пока нет
- Microbiology Progress ExamДокумент76 страницMicrobiology Progress ExamlenvycahpdelusaОценок пока нет
- Poster Emma AccorsiДокумент1 страницаPoster Emma Accorsisagun maharjanОценок пока нет
- Jurnal Formulasi Krim Gentamisin SulfatДокумент15 страницJurnal Formulasi Krim Gentamisin SulfatNandea Zulfana HendrawanОценок пока нет
- Interpretation Guide PDFДокумент6 страницInterpretation Guide PDFCaecilia Jessica UnarsoОценок пока нет
- ESCRS EndophthalmitisДокумент52 страницыESCRS EndophthalmitisKaveh Vahdani100% (2)