Вам также может понравиться
- Arch Ophthalmol 1991 YannuzziДокумент6 страницArch Ophthalmol 1991 YannuzziremotmОценок пока нет
- Am J Ophthalmol 2015 SridharДокумент12 страницAm J Ophthalmol 2015 SridharremotmОценок пока нет
- Am J Ophthalmol 2014 YuДокумент13 страницAm J Ophthalmol 2014 YuremotmОценок пока нет
- Am J Ophthalmol 2015 DansinganiДокумент5 страницAm J Ophthalmol 2015 DansinganiremotmОценок пока нет
- Am J Ophthalmol 2015 ChenДокумент10 страницAm J Ophthalmol 2015 ChenremotmОценок пока нет
- Arch Ophthalmol 2011 YehДокумент4 страницыArch Ophthalmol 2011 YehremotmОценок пока нет
- Am J Ophthalmol 2014 Rahimy-3Документ10 страницAm J Ophthalmol 2014 Rahimy-3remotmОценок пока нет
- AJOPHT 1978 PriluckДокумент4 страницыAJOPHT 1978 PriluckremotmОценок пока нет
- Acta Ophthalmol Scand 2000 Feigl-1Документ4 страницыActa Ophthalmol Scand 2000 Feigl-1remotmОценок пока нет
- Squisis MacularДокумент8 страницSquisis MacularremotmОценок пока нет
- Ajopht 1977 RushДокумент5 страницAjopht 1977 RushremotmОценок пока нет
- Brief Reports Out - 2001Документ39 страницBrief Reports Out - 2001remotmОценок пока нет
- Choroidal Granulomas in Sistemic SarcoidosisДокумент8 страницChoroidal Granulomas in Sistemic SarcoidosisremotmОценок пока нет
- Artigo01 10 - 3928 - 1081597X - 20120921 - 07Документ11 страницArtigo01 10 - 3928 - 1081597X - 20120921 - 07remotmОценок пока нет
- Brief Reports Fev - .2001pdfДокумент30 страницBrief Reports Fev - .2001pdfremotmОценок пока нет
- AntioxidantДокумент8 страницAntioxidantremotmОценок пока нет
- Acute Multifocal Placoid Pigment EpitheliopathyДокумент8 страницAcute Multifocal Placoid Pigment EpitheliopathyremotmОценок пока нет
- Artigo 03 Eye201122aДокумент5 страницArtigo 03 Eye201122aremotmОценок пока нет
- An Analysis of Lesion Size and Location in Newly Diagnosed CyДокумент7 страницAn Analysis of Lesion Size and Location in Newly Diagnosed CyremotmОценок пока нет
- A Randomized, Double-Masked Trial of Topical Ketorolac VersusДокумент6 страницA Randomized, Double-Masked Trial of Topical Ketorolac VersusremotmОценок пока нет
- Katarak Penyebab KebutaanДокумент96 страницKatarak Penyebab KebutaanIhsan HaidarОценок пока нет
- Oral Mifepristone For Chronic Central Serous.26Документ9 страницOral Mifepristone For Chronic Central Serous.26remotmОценок пока нет
- Spaide PDFДокумент11 страницSpaide PDFremotmОценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Pyro ShieldДокумент6 страницPyro Shieldmunim87Оценок пока нет
- Contemp World Module 2 Topics 1 4Документ95 страницContemp World Module 2 Topics 1 4Miguel EderОценок пока нет
- Government of India Act 1858Документ3 страницыGovernment of India Act 1858AlexitoОценок пока нет
- Singapore Electricity MarketДокумент25 страницSingapore Electricity MarketTonia GlennОценок пока нет
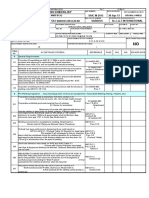
- WPGPipingIndex Form 167 PDFДокумент201 страницаWPGPipingIndex Form 167 PDFRaj AryanОценок пока нет
- Mathematical Geophysics: Class One Amin KhalilДокумент13 страницMathematical Geophysics: Class One Amin KhalilAmin KhalilОценок пока нет
- A Perspective Study On Fly Ash-Lime-Gypsum Bricks and Hollow Blocks For Low Cost Housing DevelopmentДокумент7 страницA Perspective Study On Fly Ash-Lime-Gypsum Bricks and Hollow Blocks For Low Cost Housing DevelopmentNadiah AUlia SalihiОценок пока нет
- Crivit IAN 89192 FlashlightДокумент2 страницыCrivit IAN 89192 FlashlightmОценок пока нет
- 1.6 Program AdministrationДокумент56 страниц1.6 Program Administration'JeoffreyLaycoОценок пока нет
- Starrett 3812Документ18 страницStarrett 3812cdokepОценок пока нет
- SCHEDULE OF FEES - FinalДокумент1 страницаSCHEDULE OF FEES - FinalAbhishek SunaОценок пока нет
- I5386-Bulk SigmaДокумент1 страницаI5386-Bulk SigmaCleaver BrightОценок пока нет
- Karmex 80df Diuron MsdsДокумент9 страницKarmex 80df Diuron MsdsSouth Santee Aquaculture100% (1)
- WVU's Response Letter To Campbell Regarding HugginsДокумент4 страницыWVU's Response Letter To Campbell Regarding HugginsJosh JarnaginОценок пока нет
- Summary - A Short Course On Swing TradingДокумент2 страницыSummary - A Short Course On Swing TradingsumonОценок пока нет
- Statable 1Документ350 страницStatable 1Shelly SantiagoОценок пока нет
- Saic-M-2012 Rev 7 StructureДокумент6 страницSaic-M-2012 Rev 7 StructuremohamedqcОценок пока нет
- Mayor Breanna Lungo-Koehn StatementДокумент2 страницыMayor Breanna Lungo-Koehn StatementNell CoakleyОценок пока нет
- Corporation Law Review Test Midterms 2019Документ4 страницыCorporation Law Review Test Midterms 2019Van NessaОценок пока нет
- Types of Electrical Protection Relays or Protective RelaysДокумент7 страницTypes of Electrical Protection Relays or Protective RelaysTushar SinghОценок пока нет
- Procurement Audit PlanДокумент12 страницProcurement Audit PlanMustafa Bilal100% (1)
- Rhino HammerДокумент4 страницыRhino HammerMichael BОценок пока нет
- Coca-Cola Summer Intern ReportДокумент70 страницCoca-Cola Summer Intern ReportSourabh NagpalОценок пока нет
- Vocabulary Practice Unit 8Документ4 страницыVocabulary Practice Unit 8José PizarroОценок пока нет
- CENT - Company Presentation Q1 2020 PDFДокумент22 страницыCENT - Company Presentation Q1 2020 PDFsabrina rahmawatiОценок пока нет
- Strategic Management ModelsДокумент4 страницыStrategic Management ModelsBarno NicholusОценок пока нет
- Hoja Tecnica Item 2 DRC-9-04X12-D-H-D UV BK LSZH - F904804Q6B PDFДокумент2 страницыHoja Tecnica Item 2 DRC-9-04X12-D-H-D UV BK LSZH - F904804Q6B PDFMarco Antonio Gutierrez PulchaОценок пока нет
- Study of Means End Value Chain ModelДокумент19 страницStudy of Means End Value Chain ModelPiyush Padgil100% (1)
- SWOT AnalysisДокумент6 страницSWOT AnalysisSSPK_92Оценок пока нет
- h6811 Datadomain DsДокумент5 страницh6811 Datadomain DsChristian EstebanОценок пока нет