Вам также может понравиться
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Pudendal Neuralgia and HomoeopathyДокумент14 страницPudendal Neuralgia and HomoeopathyDr. Rajneesh Kumar Sharma MD HomОценок пока нет
- Polycythemia Vera and HomoeopathyДокумент25 страницPolycythemia Vera and HomoeopathyDr. Rajneesh Kumar Sharma MD Hom100% (2)
- Koko KirjaДокумент155 страницKoko KirjaMihaaaОценок пока нет
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Vitamin D Intoxication and HomoeopathyДокумент19 страницVitamin D Intoxication and HomoeopathyDr. Rajneesh Kumar Sharma MD HomОценок пока нет
- Hypersexuality and HomoeopathyДокумент10 страницHypersexuality and HomoeopathyDr. Rajneesh Kumar Sharma MD Hom100% (1)
- Burning Mouth Syndrome and HomoeopathyДокумент12 страницBurning Mouth Syndrome and HomoeopathyDr. Rajneesh Kumar Sharma MD HomОценок пока нет
- Abdominal Migraine and HomoeopathyДокумент17 страницAbdominal Migraine and HomoeopathyDr. Rajneesh Kumar Sharma MD HomОценок пока нет
- Growth and Development of Cranial and Facial RegionДокумент81 страницаGrowth and Development of Cranial and Facial RegionSwati PawarОценок пока нет
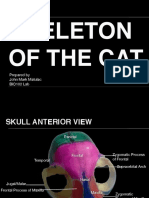
- Skeleton of The Cat: Prepared by John Mark Matulac BIO102 LabДокумент27 страницSkeleton of The Cat: Prepared by John Mark Matulac BIO102 LabJoachimОценок пока нет
- Painful Penile Induration and HomoeopathyДокумент12 страницPainful Penile Induration and HomoeopathyDr. Rajneesh Kumar Sharma MD HomОценок пока нет
- Laboratory 7Документ8 страницLaboratory 7Diana Rose SaludoОценок пока нет
- Human Remains Documentation PacketДокумент22 страницыHuman Remains Documentation Packetselk_namОценок пока нет
- Dermatitis and HomoeopathyДокумент18 страницDermatitis and HomoeopathyDr. Rajneesh Kumar Sharma MD Hom100% (1)
- Compulsive Buying Disorder and HomoeopathyДокумент7 страницCompulsive Buying Disorder and HomoeopathyDr. Rajneesh Kumar Sharma MD Hom100% (1)
- Munchausen Syndrome and HomoeopathyДокумент10 страницMunchausen Syndrome and HomoeopathyDr. Rajneesh Kumar Sharma MD HomОценок пока нет
- Bartter Syndrome, Gitelman Syndrome and HomoeopathyДокумент12 страницBartter Syndrome, Gitelman Syndrome and HomoeopathyDr. Rajneesh Kumar Sharma MD HomОценок пока нет
- Dwnload Full Mastering Healthcare Terminology e Book Ebook PDFДокумент51 страницаDwnload Full Mastering Healthcare Terminology e Book Ebook PDFkevin.larson517100% (31)
- Headand NeckNeck and Head RadiologyДокумент69 страницHeadand NeckNeck and Head RadiologyvsignatureОценок пока нет
- Vol I - Oase, Articulatii, Ligamente Si Muschi PDFДокумент454 страницыVol I - Oase, Articulatii, Ligamente Si Muschi PDFBianca Byby100% (1)
- The Brain Fag Syndrome and HomoeopathyДокумент8 страницThe Brain Fag Syndrome and HomoeopathyDr. Rajneesh Kumar Sharma MD HomОценок пока нет
- Lipoma and HomoeopathyДокумент12 страницLipoma and HomoeopathyDr. Rajneesh Kumar Sharma MD HomОценок пока нет
- Exercise 4: Skeletal SystemДокумент8 страницExercise 4: Skeletal SystemstevemacabsОценок пока нет
- Pseudobulbar Affect and HomoeopathyДокумент13 страницPseudobulbar Affect and HomoeopathyDr. Rajneesh Kumar Sharma MD HomОценок пока нет
- A Case of Postpartum HemorrhageДокумент10 страницA Case of Postpartum HemorrhageDr. Rajneesh Kumar Sharma MD HomОценок пока нет
- PNDS and HomoeopathyДокумент8 страницPNDS and HomoeopathyDr. Rajneesh Kumar Sharma MD Hom100% (1)
- Role of Homoeopathy in Vitamin D Deficiency Induced Psychotic DisordersДокумент19 страницRole of Homoeopathy in Vitamin D Deficiency Induced Psychotic DisordersDr. Rajneesh Kumar Sharma MD HomОценок пока нет
- Waardenburg Syndrome and HomoeopathyДокумент11 страницWaardenburg Syndrome and HomoeopathyDr. Rajneesh Kumar Sharma MD HomОценок пока нет
- Kleptomania and HomoeopathyДокумент7 страницKleptomania and HomoeopathyDr. Rajneesh Kumar Sharma MD HomОценок пока нет
- Pheochromocytoma and HomoeopathyДокумент13 страницPheochromocytoma and HomoeopathyDr. Rajneesh Kumar Sharma MD HomОценок пока нет
- Stickler Syndrome and HomoeopathyДокумент9 страницStickler Syndrome and HomoeopathyDr. Rajneesh Kumar Sharma MD HomОценок пока нет
- Hirayama Disease and HomoeopathyДокумент11 страницHirayama Disease and HomoeopathyDr. Rajneesh Kumar Sharma MD Hom100% (3)
- Smoking and HomoeopathyДокумент13 страницSmoking and Homoeopathydrrajneeshhom7658Оценок пока нет
- Pain and HomoeopathyДокумент12 страницPain and HomoeopathyDr. Rajneesh Kumar Sharma MD HomОценок пока нет
- Confusion and HomoeopathyДокумент22 страницыConfusion and HomoeopathyDr. Rajneesh Kumar Sharma MD HomОценок пока нет
- Darier Disease and HomoeopathyДокумент10 страницDarier Disease and HomoeopathyDr. Rajneesh Kumar Sharma MD HomОценок пока нет
- Nausea During Teeth Brushing and HomoeopathyДокумент7 страницNausea During Teeth Brushing and HomoeopathyDr. Rajneesh Kumar Sharma MD Hom100% (1)
- Microscopic Polyangiitis and HomoeopathyДокумент16 страницMicroscopic Polyangiitis and HomoeopathyDr. Rajneesh Kumar Sharma MD HomОценок пока нет
- Intracranial Hypertensionand HomoeopathyДокумент14 страницIntracranial Hypertensionand HomoeopathyDr. Rajneesh Kumar Sharma MD HomОценок пока нет
- Trochanteric Bursitis and HomoeopathyДокумент5 страницTrochanteric Bursitis and HomoeopathyDr. Rajneesh Kumar Sharma MD Hom100% (1)
- Zygomatico-Maxillary OsteotomyДокумент8 страницZygomatico-Maxillary Osteotomypratiksha malhotraОценок пока нет
- Wa0001Документ14 страницWa0001adityo wibhisonoОценок пока нет
- Cadena2015LeyvachelysRed PDFДокумент25 страницCadena2015LeyvachelysRed PDFEdwin CadenaОценок пока нет
- Norma Basalis: External Aspect of The Cranial BaseДокумент14 страницNorma Basalis: External Aspect of The Cranial BaseBahadur Baloch100% (1)
- Chapter 11 - The Appendicular Skeletal SystemДокумент6 страницChapter 11 - The Appendicular Skeletal Systemmedianoche191% (11)
- Typical Long BonesДокумент25 страницTypical Long Bonesamit1kumar1barmanОценок пока нет
- Praktikum Tulang Dan Sendi 2Документ10 страницPraktikum Tulang Dan Sendi 2Andalas FotocopyОценок пока нет
- Daftar KolomДокумент28 страницDaftar KolomViaОценок пока нет
- Human Skeleton InstructionsДокумент2 страницыHuman Skeleton InstructionsCine Wanka NemfiusfilmsОценок пока нет
- Handouts in Skeletal SystemДокумент6 страницHandouts in Skeletal SystemShiela Mae EslumОценок пока нет
- Presented By:-Dr. Sushma Tomar Associate Professor Department of AnatomyДокумент20 страницPresented By:-Dr. Sushma Tomar Associate Professor Department of AnatomyCristine EchaveОценок пока нет
- Kunci SL 2 Extremitas Inferior PDFДокумент9 страницKunci SL 2 Extremitas Inferior PDFGisela MurdanyОценок пока нет
- Os FrontaleДокумент1 страницаOs FrontaleLBllb lblОценок пока нет
- Medial MaxillectomyДокумент12 страницMedial MaxillectomyJamesОценок пока нет
- 7.2 Bone Markings - Anatomy & PhysiologyДокумент1 страница7.2 Bone Markings - Anatomy & PhysiologydonaldooiОценок пока нет
- Anatomy Muscles of CatДокумент67 страницAnatomy Muscles of Cathgfree41392Оценок пока нет
- Jenisie Pasigan - Ch. 8-2 - Skeletal System Notes Packet (Part II)Документ5 страницJenisie Pasigan - Ch. 8-2 - Skeletal System Notes Packet (Part II)Jenisie PasiganОценок пока нет
- Anatomy Bones and SkeletonДокумент4 страницыAnatomy Bones and Skeletonタナトス ThanatosОценок пока нет
- The Skeletal System Human Body (206) Axial Skeleton (80) Skull (28) A. Paired Bones (11x2 22)Документ17 страницThe Skeletal System Human Body (206) Axial Skeleton (80) Skull (28) A. Paired Bones (11x2 22)Leo Cordel Jr.Оценок пока нет
- 7 Bone Structure Labeling Review 1Документ34 страницы7 Bone Structure Labeling Review 1api-242868690Оценок пока нет
- Fractures With Eponyms-Cl. OrthoДокумент6 страницFractures With Eponyms-Cl. OrthoYarra Sri HarikaОценок пока нет