Вам также может понравиться
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (894)
- Abdomen - FRCEM SuccessДокумент275 страницAbdomen - FRCEM SuccessAbin ThomasОценок пока нет
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Rapid Prep Easy To Read HandoutДокумент473 страницыRapid Prep Easy To Read HandoutTina Moore93% (15)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- EP - EngineДокумент4 страницыEP - EngineAkhmad HasimОценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- PC3 The Sea PeopleДокумент100 страницPC3 The Sea PeoplePJ100% (4)
- Ncps GeriatricsДокумент6 страницNcps GeriatricsKathrina CraveОценок пока нет
- Elevator Traction Machine CatalogДокумент24 страницыElevator Traction Machine CatalogRafif100% (1)
- Understanding Stevens-Johnson Syndrome (SJSДокумент53 страницыUnderstanding Stevens-Johnson Syndrome (SJSKathrina CraveОценок пока нет
- Extended Care: Related ConcernsДокумент29 страницExtended Care: Related ConcernsKathrina Crave100% (1)
- (Razavi) Design of Analog Cmos Integrated CircuitsДокумент21 страница(Razavi) Design of Analog Cmos Integrated CircuitsNiveditha Nivi100% (1)
- Gautam Samhita CHP 1 CHP 2 CHP 3 ColorДокумент22 страницыGautam Samhita CHP 1 CHP 2 CHP 3 ColorSaptarishisAstrology100% (1)
- Artifact and Thingamy by David MitchellДокумент8 страницArtifact and Thingamy by David MitchellPedro PriorОценок пока нет
- Interactive Architecture Adaptive WorldДокумент177 страницInteractive Architecture Adaptive Worldhoma massihaОценок пока нет
- Regarding The CaseДокумент3 страницыRegarding The CaseKathrina CraveОценок пока нет
- K. Patho NarrativeДокумент3 страницыK. Patho NarrativeKathrina CraveОценок пока нет
- Pearl of AllahДокумент1 страницаPearl of AllahKathrina CraveОценок пока нет
- The Crowne Inn InfoДокумент4 страницыThe Crowne Inn InfoKathrina CraveОценок пока нет
- BiostatДокумент2 страницыBiostattharinasalvatoreОценок пока нет
- HumanitiesДокумент1 страницаHumanitiesKathrina CraveОценок пока нет
- Generic Name Brand NameДокумент7 страницGeneric Name Brand NameKathrina CraveОценок пока нет
- Smoking 1232Документ44 страницыSmoking 1232Kathrina CraveОценок пока нет
- Rotational Budgeting: Gross Income Percentage of Income SpentДокумент1 страницаRotational Budgeting: Gross Income Percentage of Income SpentKathrina CraveОценок пока нет
- Dressing 08293Документ17 страницDressing 08293Kathrina CraveОценок пока нет
- Quiz in History123223Документ2 страницыQuiz in History123223Kathrina CraveОценок пока нет
- Written Report1232334Документ6 страницWritten Report1232334Kathrina CraveОценок пока нет
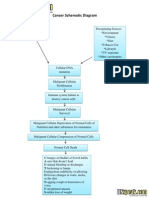
- Cancer Schematic DiagramДокумент1 страницаCancer Schematic DiagramJonathan ObañaОценок пока нет
- Postpartum Physical Assessment ParametersДокумент5 страницPostpartum Physical Assessment ParametersKathrina CraveОценок пока нет
- Answer KeyДокумент3 страницыAnswer KeyKathrina CraveОценок пока нет
- Assess 8 PointДокумент3 страницыAssess 8 PointKathrina CraveОценок пока нет
- Table 1Документ3 страницыTable 1Kathrina CraveОценок пока нет
- Benign Prostatic HyperplasiaДокумент9 страницBenign Prostatic Hyperplasiamardsz100% (1)
- DYSRHYTHMIAS123Документ17 страницDYSRHYTHMIAS123Kathrina CraveОценок пока нет
- ICP Monitoring: Embedded HyperlinksДокумент15 страницICP Monitoring: Embedded HyperlinksKathrina CraveОценок пока нет
- AlcoholismДокумент32 страницыAlcoholismKathrina CraveОценок пока нет
- 12, Single Spacing: Review of LiteratureДокумент2 страницы12, Single Spacing: Review of LiteratureKathrina CraveОценок пока нет
- Postpartum Physical Assessment ParametersДокумент5 страницPostpartum Physical Assessment ParametersKathrina CraveОценок пока нет
- List of Tables TemplateДокумент2 страницыList of Tables TemplateKathrina CraveОценок пока нет
- NCPДокумент4 страницыNCPKathrina CraveОценок пока нет
- Albert Bandura Developmental TheoryДокумент1 страницаAlbert Bandura Developmental TheoryKathrina CraveОценок пока нет
- Cola IzziДокумент1 страницаCola IzziKathrina CraveОценок пока нет
- Introduction To Finite Element Methods (2001) (En) (489s)Документ489 страницIntroduction To Finite Element Methods (2001) (En) (489s)green77parkОценок пока нет
- Monodisperse Droplet Generators As Potential Atomizers For Spray Drying Technology PDFДокумент11 страницMonodisperse Droplet Generators As Potential Atomizers For Spray Drying Technology PDFfishvalОценок пока нет
- Revolutionizing Energy Harvesting Harnessing Ambient Solar Energy For Enhanced Electric Power GenerationДокумент14 страницRevolutionizing Energy Harvesting Harnessing Ambient Solar Energy For Enhanced Electric Power GenerationKIU PUBLICATION AND EXTENSIONОценок пока нет
- Final Decision W - Cover Letter, 7-14-22Документ19 страницFinal Decision W - Cover Letter, 7-14-22Helen BennettОценок пока нет
- FP-XH PGRG eДокумент936 страницFP-XH PGRG ebvladimirov85Оценок пока нет
- O2 Orthodontic Lab Catalog PDFДокумент20 страницO2 Orthodontic Lab Catalog PDFplayer osamaОценок пока нет
- Mechanical Specifications For Fiberbond ProductДокумент8 страницMechanical Specifications For Fiberbond ProducthasnizaОценок пока нет
- Air Wellness QRSДокумент2 страницыAir Wellness QRSapi-3743459Оценок пока нет
- Plate-Load TestДокумент20 страницPlate-Load TestSalman LakhoОценок пока нет
- JUPITER 9000K H1PreliminaryДокумент1 страницаJUPITER 9000K H1PreliminaryMarian FlorescuОценок пока нет
- Uhf Leaky Feeder Rev CДокумент4 страницыUhf Leaky Feeder Rev CLuis Isaac PadillaОценок пока нет
- Cyclograph User ManualДокумент15 страницCyclograph User ManualPeter BateОценок пока нет
- Fundermax Exterior Technic 2011gb WebДокумент88 страницFundermax Exterior Technic 2011gb WebarchpavlovicОценок пока нет
- A Fossil Hunting Guide To The Tertiary Formations of Qatar, Middle-EastДокумент82 страницыA Fossil Hunting Guide To The Tertiary Formations of Qatar, Middle-EastJacques LeBlanc100% (18)
- Flowing Gas Material BalanceДокумент4 страницыFlowing Gas Material BalanceVladimir PriescuОценок пока нет
- HVCCI UPI Form No. 3 Summary ReportДокумент2 страницыHVCCI UPI Form No. 3 Summary ReportAzumi AyuzawaОценок пока нет
- Lesson Plan: Lesson: Projectiles Without Air ResistanceДокумент4 страницыLesson Plan: Lesson: Projectiles Without Air ResistanceeltytanОценок пока нет
- Qualitative Research EssayДокумент9 страницQualitative Research EssayMichael FoleyОценок пока нет
- PDFViewer - JSP 3Документ46 страницPDFViewer - JSP 3Kartik ChaudharyОценок пока нет
- TIA Selection Tool: Release Notes V2022.05Документ10 страницTIA Selection Tool: Release Notes V2022.05Patil Amol PandurangОценок пока нет
- Fraktur Dentoalevolar (Yayun)Документ22 страницыFraktur Dentoalevolar (Yayun)Gea RahmatОценок пока нет