Вам также может понравиться
- Hem311 Week 13 Lab - Reticulocyte CountДокумент32 страницыHem311 Week 13 Lab - Reticulocyte CountSheine EspinoОценок пока нет
- Ana IfДокумент101 страницаAna Ifshrikrishnapathlab100% (1)
- Bacte TestДокумент10 страницBacte TestRiondalionОценок пока нет
- Blood Morphometry or Blood Film CommentДокумент103 страницыBlood Morphometry or Blood Film CommentYangnuu TitusОценок пока нет
- Identification of Normal and Abnormal Forms of RedДокумент32 страницыIdentification of Normal and Abnormal Forms of RedNada hasanОценок пока нет
- COMPLETE BLOOD COUNT Lecture GuideДокумент9 страницCOMPLETE BLOOD COUNT Lecture GuideKaycee Gretz LorescaОценок пока нет
- 1 Blood SmearДокумент59 страниц1 Blood SmearGabi Tim100% (1)
- Microscopic Exam 01 - RBC, WBC, BacteriaДокумент30 страницMicroscopic Exam 01 - RBC, WBC, BacteriaBrent LagartoОценок пока нет
- Hema II Chapter11 - QA in HematologyДокумент29 страницHema II Chapter11 - QA in HematologyAmanuel MaruОценок пока нет
- Coagulation NotesДокумент14 страницCoagulation NotesthrowawyОценок пока нет
- 1 Introduction To AnemiaДокумент60 страниц1 Introduction To AnemiaKhisha RangasОценок пока нет
- Hematology 2 TEST QUESTIONSДокумент4 страницыHematology 2 TEST QUESTIONSa a r o n b a u t i s t aОценок пока нет
- Correctly: IncorrectlyДокумент70 страницCorrectly: IncorrectlyDjdjjd Siisus100% (1)
- Types Of Hemolytic Anemia, A Simple Guide To The Condition, Treatment And Related ConditionsОт EverandTypes Of Hemolytic Anemia, A Simple Guide To The Condition, Treatment And Related ConditionsОценок пока нет
- Molecular Diagnosis in HaematologyДокумент23 страницыMolecular Diagnosis in HaematologyUmar'Farouq Oni100% (1)
- Manual Platelet CountДокумент14 страницManual Platelet CountMiyo SobremisanaОценок пока нет
- Antibody IdentificationДокумент27 страницAntibody Identificationhamaada100% (1)
- Anemia and Red Blood Cell Disorder Lecture by Dr. Rosales (Nov 6, 2017)Документ7 страницAnemia and Red Blood Cell Disorder Lecture by Dr. Rosales (Nov 6, 2017)Ian Gabrielle Mercado CuynoОценок пока нет
- HematologyДокумент5 страницHematologyIvy Jan OcateОценок пока нет
- Breastfeeding and Down SyndromeДокумент239 страницBreastfeeding and Down SyndromeSim M ChangОценок пока нет
- Morphology OF Red Blood CellsДокумент36 страницMorphology OF Red Blood CellsFrancis ValdezОценок пока нет
- CC1 - Topic 1Документ11 страницCC1 - Topic 1Marie MontemarОценок пока нет
- RBCs Abnormal MorphologyДокумент33 страницыRBCs Abnormal MorphologyLailitifa Windy SОценок пока нет
- Analysis of Physical Properties of UrineДокумент2 страницыAnalysis of Physical Properties of UrineameerabestОценок пока нет
- Blood Bank (2 Week) : Antibody ScreensДокумент5 страницBlood Bank (2 Week) : Antibody ScreensAngela ReyesОценок пока нет
- Leukocyte DisordersДокумент55 страницLeukocyte DisordersSherlyn Yee100% (1)
- Autoimmune Hemolytic AnemiaДокумент55 страницAutoimmune Hemolytic AnemiaNicky SebastianОценок пока нет
- Pancytopenia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОт EverandPancytopenia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОценок пока нет
- Gel TechnologyДокумент2 страницыGel TechnologyJai Carungay100% (1)
- Laboratorial Diagnostics Keypoints RevisionДокумент6 страницLaboratorial Diagnostics Keypoints RevisionFathimathОценок пока нет
- HemoglobinopathiesДокумент3 страницыHemoglobinopathiesChatie PipitОценок пока нет
- WBC Usmle QuestionsДокумент17 страницWBC Usmle Questionssplinter594100% (1)
- Urinalysis and Body Fluids2020Документ47 страницUrinalysis and Body Fluids2020MONFOLA100% (1)
- Coagulation CascadeДокумент4 страницыCoagulation CascadezainabОценок пока нет
- CBCДокумент12 страницCBCDaNa Al-jomah100% (1)
- Red Cell and White Cell Counting, BloodДокумент89 страницRed Cell and White Cell Counting, BloodJovel GangcuangcoОценок пока нет
- Hematology Case StudyДокумент14 страницHematology Case StudyDiego GarciaОценок пока нет
- HaematologyДокумент68 страницHaematologytapoolnoОценок пока нет
- HemaДокумент59 страницHemaSteph VeeОценок пока нет
- Hematology QuizДокумент5 страницHematology Quizkep1313100% (1)
- Wintrobe Test PDFДокумент9 страницWintrobe Test PDFMaria Chacón CarbajalОценок пока нет
- HAEMOPOIESISДокумент6 страницHAEMOPOIESISDiyana ZahariОценок пока нет
- Clearance and GFR: Major DR Arabinda Mohan Bhattarai Lecturer (Biochemistry), NAIHSДокумент25 страницClearance and GFR: Major DR Arabinda Mohan Bhattarai Lecturer (Biochemistry), NAIHSChandan SahОценок пока нет
- Lab 2 ImmunohaematologyДокумент3 страницыLab 2 ImmunohaematologyLorraine ThompsonОценок пока нет
- Study Questions (Hematology)Документ11 страницStudy Questions (Hematology)tkanesОценок пока нет
- Clinical Pathology 3-6 UrinalysisДокумент3 страницыClinical Pathology 3-6 UrinalysisAndrew KalawОценок пока нет
- HematologyДокумент4 страницыHematologyliesel_12Оценок пока нет
- BOC Study Guide: The MostДокумент17 страницBOC Study Guide: The MostDeanne LambanОценок пока нет
- CytochemistryДокумент55 страницCytochemistrySaad Zafar Awan100% (1)
- Chapter 14 - Routine and Point of Care Testing in HematologyДокумент10 страницChapter 14 - Routine and Point of Care Testing in HematologyNathaniel Sim100% (1)
- Incorrectly: CorrectlyДокумент25 страницIncorrectly: CorrectlypikachuОценок пока нет
- Disorders of Iron Kinetics and Heme MetabolismДокумент12 страницDisorders of Iron Kinetics and Heme MetabolismJoanne JardinОценок пока нет
- CYTOCHEMISTRY by Brian M. Denney, RMT: PhosphatasesДокумент5 страницCYTOCHEMISTRY by Brian M. Denney, RMT: PhosphatasesHarvy Halasan0% (1)
- CBC Reviewer Anaphy LabДокумент9 страницCBC Reviewer Anaphy LabARVINE JUSTINE CORPUZОценок пока нет
- RBC MembraneДокумент41 страницаRBC MembranemwambungupОценок пока нет
- WBC AbN MorphologyДокумент2 страницыWBC AbN MorphologyTristan Iris100% (2)
- All Objectives HematologyДокумент45 страницAll Objectives HematologyNursing200980% (5)
- 04.28 Hematology PPT NotesДокумент6 страниц04.28 Hematology PPT Notesmlttechnologist9Оценок пока нет
- Cell Inclusions: John SantangeloДокумент45 страницCell Inclusions: John Santangelosaint5470Оценок пока нет
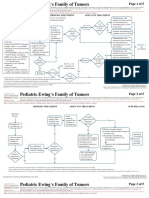
- Ca Treatment Ewings Pedi Web AlgorithmДокумент5 страницCa Treatment Ewings Pedi Web AlgorithmSim M ChangОценок пока нет
- 1 IntroductionДокумент1 страница1 IntroductionSim M ChangОценок пока нет
- Your Babyand DSДокумент2 страницыYour Babyand DSSim M ChangОценок пока нет
- ClaudicationДокумент10 страницClaudicationSim M ChangОценок пока нет
- Approach To NB With ThrombocytopeniaДокумент7 страницApproach To NB With ThrombocytopeniaSim M ChangОценок пока нет
- Hip Fractures: Types of Fracture and AnatomyДокумент9 страницHip Fractures: Types of Fracture and AnatomySim M ChangОценок пока нет
- AAP Palivizumab ProphylaxisДокумент9 страницAAP Palivizumab ProphylaxisSim M ChangОценок пока нет
- A Trial of Imaging Selection and Endovascular Treatment For Ischemic StrokeДокумент10 страницA Trial of Imaging Selection and Endovascular Treatment For Ischemic StrokeSim M ChangОценок пока нет
- MyocarditisДокумент2 страницыMyocarditisSim M ChangОценок пока нет
- Achalasia: A Hard Diagnosis To Swallow Simone Chang Dr. Bascombe and Dr. MehotraДокумент12 страницAchalasia: A Hard Diagnosis To Swallow Simone Chang Dr. Bascombe and Dr. MehotraSim M ChangОценок пока нет
- Staphylococcus EpidermidisДокумент12 страницStaphylococcus EpidermidisSim M ChangОценок пока нет