Вам также может понравиться
- Diabetes Mellitus CPGДокумент157 страницDiabetes Mellitus CPGejikieru03100% (3)
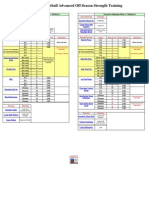
- Workout - Sheet - Football Advanced Off-Season Strength TrainingДокумент18 страницWorkout - Sheet - Football Advanced Off-Season Strength TrainingTom HochhalterОценок пока нет
- Strength Training Guidelines and PrinciplesДокумент4 страницыStrength Training Guidelines and Principlessalva1310Оценок пока нет
- How To Lose Weight 10 Lbs in A Month: - 7 Simple StepsДокумент26 страницHow To Lose Weight 10 Lbs in A Month: - 7 Simple StepsRahmad RizkiОценок пока нет
- Diabetes PPT FianlДокумент31 страницаDiabetes PPT FianlUqba MishalОценок пока нет
- Birthmarks Identificationandmx201205ryanДокумент4 страницыBirthmarks Identificationandmx201205ryanDanielcc LeeОценок пока нет
- 14 Essentials To Assessment and Care PlanMT2013!08!018-BRODATY - 0Документ9 страниц14 Essentials To Assessment and Care PlanMT2013!08!018-BRODATY - 0Danielcc Lee100% (1)
- Blood Transfusion ProcedureДокумент0 страницBlood Transfusion ProcedureDanielcc LeeОценок пока нет
- Diabetic Ketoacidosis Case PresentationДокумент37 страницDiabetic Ketoacidosis Case PresentationNathan Vince Cruz100% (2)
- GeriatricsДокумент12 страницGeriatricsDanielcc Lee100% (1)
- Clinical Chemistry Case AnalysisДокумент6 страницClinical Chemistry Case Analysisaliana100% (5)
- Diabetes Mellitus IIДокумент20 страницDiabetes Mellitus IIMa R Dy100% (1)
- Types of Therapeutic DietsДокумент10 страницTypes of Therapeutic DietsFaith Marfil100% (1)
- Benefits of Carrot JuiceДокумент0 страницBenefits of Carrot JuiceeQualizerОценок пока нет
- Capillary Blood GlucoseДокумент4 страницыCapillary Blood GlucoseDennis CobbОценок пока нет
- Section 2. Classification and Diagnosis of DiabetesДокумент27 страницSection 2. Classification and Diagnosis of Diabetesbidbid88Оценок пока нет
- A Practical Guide To Diagnosing Type 2 DiabetesДокумент4 страницыA Practical Guide To Diagnosing Type 2 Diabeteselena_bautista_3Оценок пока нет
- Update On: Diabetes MellitusДокумент37 страницUpdate On: Diabetes MellitusDr. Mamunul Abedin100% (1)
- Laboratory Diagnosis and Monitoring Type 2 Diabetes Mellitus - SEKAR EMSДокумент29 страницLaboratory Diagnosis and Monitoring Type 2 Diabetes Mellitus - SEKAR EMSRaja Iqbal Mulya HarahapОценок пока нет
- (Osborn) Chapter 53 Learning Outcomes (Number and Title)Документ33 страницы(Osborn) Chapter 53 Learning Outcomes (Number and Title)Kitties100% (1)
- Diagnosis and Management of Type 2 Diabetes Mellitus ©stephen D. Sisson MD/Ambulatory Curriculum 2021Документ48 страницDiagnosis and Management of Type 2 Diabetes Mellitus ©stephen D. Sisson MD/Ambulatory Curriculum 2021Carolina González RiveraОценок пока нет
- Diagnosis of Gestational Diabetes MellitusДокумент2 страницыDiagnosis of Gestational Diabetes Mellitusamulan_aОценок пока нет
- Mellitus/ Section 1: Epidemiology and AetiologyДокумент52 страницыMellitus/ Section 1: Epidemiology and AetiologybimackpbgtОценок пока нет
- SGD 3: CASE DIABETES: "A Sweet Way To Lose Weight": Guide QuestionsДокумент5 страницSGD 3: CASE DIABETES: "A Sweet Way To Lose Weight": Guide QuestionsKaren Kaye CordovaОценок пока нет
- Clinical Practice Guidelines For Diabetes ManagementДокумент5 страницClinical Practice Guidelines For Diabetes ManagementIqbal Fida MaulanaОценок пока нет
- STATEMENTS ADIPS GDM Management GuidelinesДокумент10 страницSTATEMENTS ADIPS GDM Management Guidelineskitten garciaОценок пока нет
- 1-Definition Epidemiology and Classification of Diabetes in Children and Adolescents PDFДокумент14 страниц1-Definition Epidemiology and Classification of Diabetes in Children and Adolescents PDFFrancys Sierra FariasОценок пока нет
- Diabetes Mellitus: Zenebe N. (B Pharm, M Pharm) May, 2022Документ93 страницыDiabetes Mellitus: Zenebe N. (B Pharm, M Pharm) May, 2022The AbyssinicansОценок пока нет
- HypoglycaemiaДокумент3 страницыHypoglycaemiaAneejaa BidhaОценок пока нет
- Nfs 774 Case StudyДокумент37 страницNfs 774 Case Studyapi-533845626Оценок пока нет
- Diabetes MiellitusДокумент14 страницDiabetes MiellitusMha Mencoba BerubahОценок пока нет
- CJD July 2011 Position StatementДокумент3 страницыCJD July 2011 Position StatementJose RobledoОценок пока нет
- Clasificacion y Diagnostico de La Diabetes Guias Ada 2015Документ9 страницClasificacion y Diagnostico de La Diabetes Guias Ada 2015elizabeth salanОценок пока нет
- DMДокумент76 страницDMrose ann ayala100% (1)
- DD Metabolic SyndromeДокумент5 страницDD Metabolic SyndromeEluОценок пока нет
- Diagnosis of Diabetes MellitusДокумент23 страницыDiagnosis of Diabetes MellitusNkosinathi ShongweОценок пока нет
- 1 s2.0 S1877593409000575 Main PDFДокумент5 страниц1 s2.0 S1877593409000575 Main PDFTiya HilmawanОценок пока нет
- Measuring Blood Glucose LevelДокумент7 страницMeasuring Blood Glucose LevelHuda BehroozОценок пока нет
- Diabetes Mellitus Management of Gestational Diabetes - 280720Документ12 страницDiabetes Mellitus Management of Gestational Diabetes - 280720AddisОценок пока нет
- Dean OfficeДокумент73 страницыDean Officearief19Оценок пока нет
- Hypoglychemia AdultsДокумент32 страницыHypoglychemia AdultsshutekiОценок пока нет
- Thy Diabetica FibДокумент24 страницыThy Diabetica Fibaditzzz11Оценок пока нет
- DiabetesДокумент10 страницDiabetesFatima El HassouniОценок пока нет
- GDMДокумент3 страницыGDMErika RubionОценок пока нет
- How Often Should People With Diabetes Check Their Blood Glucose?Документ3 страницыHow Often Should People With Diabetes Check Their Blood Glucose?debabrata5976Оценок пока нет
- Diagnosis and Classification of Diabetes Mellitus - New Criteria - AAFPДокумент10 страницDiagnosis and Classification of Diabetes Mellitus - New Criteria - AAFPGali Alfaro ZagalОценок пока нет
- Diabetes Mellitus of The Human Digestive SystemДокумент7 страницDiabetes Mellitus of The Human Digestive SystemCHRISTINE KARENDIОценок пока нет
- Clinical Study Regarding The Effect of NДокумент7 страницClinical Study Regarding The Effect of NcolceardoinaОценок пока нет
- Protocol 007Документ7 страницProtocol 007hatem newishyОценок пока нет
- Management of Children & Young People With A New Diagnosis of Diabetes MellitusДокумент5 страницManagement of Children & Young People With A New Diagnosis of Diabetes MellitusArslan SiddiquiОценок пока нет
- DMG Diagnosis and ManagementДокумент6 страницDMG Diagnosis and ManagementCésar MonjarásОценок пока нет
- CC2E D Ananasovski - Pre-Analytical Factors in Glucose TestingДокумент36 страницCC2E D Ananasovski - Pre-Analytical Factors in Glucose TestingSaad KhanОценок пока нет
- Glucosa 2012Документ6 страницGlucosa 2012martynbbОценок пока нет
- Chapter 50 51 Prelec Quizzes Case Studies Discussion Topis and Critical Thinking Exercises Work To Be Done..Документ8 страницChapter 50 51 Prelec Quizzes Case Studies Discussion Topis and Critical Thinking Exercises Work To Be Done..Besael BaccolОценок пока нет
- Summary of IMBR-Saud Alzahrani-08-2020Документ30 страницSummary of IMBR-Saud Alzahrani-08-2020AHMAD ALROWAILYОценок пока нет
- Introduction: Diabetes Mellitus (DM) Is The Most Common Endocrine ProblemДокумент6 страницIntroduction: Diabetes Mellitus (DM) Is The Most Common Endocrine ProblemHeribertus Andi WidagdoОценок пока нет
- Original Research Article: Vitan Patel, Minal Shastri, Nisha Gaur, Prutha Jinwala, Abhishek Y. KadamДокумент5 страницOriginal Research Article: Vitan Patel, Minal Shastri, Nisha Gaur, Prutha Jinwala, Abhishek Y. KadamTam LyОценок пока нет
- Diabetic NephropathyДокумент38 страницDiabetic NephropathyMade Widiastika100% (1)
- Oral Glucose Tolerance TestДокумент6 страницOral Glucose Tolerance TestIka HabelОценок пока нет
- ADA 2010 Clinical Practice Guidelines - Revisions & Updates: Diagnosis of DiabetesДокумент6 страницADA 2010 Clinical Practice Guidelines - Revisions & Updates: Diagnosis of Diabetesหนึ่งฤทัย ไชยโยราชОценок пока нет
- Dental Management of Patients With Diabetes MellitusДокумент8 страницDental Management of Patients With Diabetes Mellitusاحمد سلامОценок пока нет
- Diabetes AwarenessДокумент37 страницDiabetes AwarenessEkalaivanОценок пока нет
- Diabetes DXДокумент17 страницDiabetes DXERICKA ODILY FLORES VALENCIAОценок пока нет
- Ajcpath112 0665Документ10 страницAjcpath112 0665RiyanОценок пока нет
- Gestational Diabetes Mellitus (GDM) .TriceДокумент47 страницGestational Diabetes Mellitus (GDM) .TricejerrydanfordfxОценок пока нет
- A. Patient's InformationДокумент8 страницA. Patient's InformationCamille Quilao PantoniОценок пока нет
- Diabetes Mellitus: Is Type Surgical Disease?Документ10 страницDiabetes Mellitus: Is Type Surgical Disease?Mateo TamayoОценок пока нет
- Canadian Journal of Diabetes: 2018 Clinical Practice GuidelinesДокумент9 страницCanadian Journal of Diabetes: 2018 Clinical Practice Guidelinesamar singhОценок пока нет
- Hypoglycemia in Diabetes: Pathophysiology, Prevalence, and PreventionОт EverandHypoglycemia in Diabetes: Pathophysiology, Prevalence, and PreventionОценок пока нет
- Commonrashes in Neonates201205suДокумент6 страницCommonrashes in Neonates201205suDanielcc LeeОценок пока нет
- 14 Essentials To MxMT2013!09!029-BRODATY - 0Документ11 страниц14 Essentials To MxMT2013!09!029-BRODATY - 0Danielcc LeeОценок пока нет
- Interpretation of The eGFR Jul 07Документ8 страницInterpretation of The eGFR Jul 07Danielcc LeeОценок пока нет
- Full Blood Count Apr04, DR Eva RaikДокумент7 страницFull Blood Count Apr04, DR Eva RaikDanielcc LeeОценок пока нет
- Diagnosis of Iron Deficiency and Iron Overload Nov 06Документ8 страницDiagnosis of Iron Deficiency and Iron Overload Nov 06Danielcc LeeОценок пока нет
- Elevated Ferritin What Should GP KnowДокумент5 страницElevated Ferritin What Should GP KnowDanielcc LeeОценок пока нет
- Bed Bugs: What The GP Needs To KnowДокумент5 страницBed Bugs: What The GP Needs To KnowDanielcc LeeОценок пока нет
- Antidote Administration Guidelines June2010Документ4 страницыAntidote Administration Guidelines June2010Danielcc LeeОценок пока нет
- Lipids - ReviewerДокумент5 страницLipids - ReviewerGabrielle FranciscoОценок пока нет
- Physical FitnessДокумент3 страницыPhysical FitnessJustine Ella Mae CarantoОценок пока нет
- Fitness Training Program: Program Start Date Client's Information Warm-UpДокумент2 страницыFitness Training Program: Program Start Date Client's Information Warm-UpMohamed AtefОценок пока нет
- B2 Enzymes HWKДокумент4 страницыB2 Enzymes HWKdrkhansacademyОценок пока нет
- Magnets On Ears Helped DiabeticsДокумент4 страницыMagnets On Ears Helped DiabeticshacchikkoОценок пока нет
- James PRN This One THXДокумент3 страницыJames PRN This One THXKaren MarcianoОценок пока нет
- The Benefits of Nipa HoneyДокумент2 страницыThe Benefits of Nipa HoneyAngelaAmericaCombalicerОценок пока нет
- Mnemonics On Pathology and MicrobiologyДокумент105 страницMnemonics On Pathology and MicrobiologyAyerhs Hahs67% (3)
- Ta 76 1 2013 11 22 SchwartzДокумент2 страницыTa 76 1 2013 11 22 SchwartzRagabi RezaОценок пока нет
- Physical Fitness 2Документ11 страницPhysical Fitness 2jonnoyjohnsonОценок пока нет
- Statement On Pulmonary RehabilitationДокумент24 страницыStatement On Pulmonary RehabilitationDavidMorenoTovarОценок пока нет
- CC CCCCC: Y CCC CCCC CCCCC CCCC CCC CCCCCCCCCC CC CДокумент3 страницыCC CCCCC: Y CCC CCCC CCCCC CCCC CCC CCCCCCCCCC CC CRachel Ann BatayolaОценок пока нет
- Institutional Case StudyДокумент4 страницыInstitutional Case StudyIrene DalisayОценок пока нет
- The Different Therapeutic Choices With Arbs. Which One To Give? When? Why?Документ12 страницThe Different Therapeutic Choices With Arbs. Which One To Give? When? Why?Jonathan Ian ArinsolОценок пока нет
- Using Uv Spectrophotometric Method To Determine The Linearity of Vildagliptin (VLD) Brands.Документ4 страницыUsing Uv Spectrophotometric Method To Determine The Linearity of Vildagliptin (VLD) Brands.Alex American-ajiras BrondОценок пока нет
- Cycling Benefits: Cycling Health and FitnessДокумент1 страницаCycling Benefits: Cycling Health and FitnessAnupam BaliОценок пока нет
- Week 6 Facilitator Copy Week 06 Renal Failure PDFДокумент7 страницWeek 6 Facilitator Copy Week 06 Renal Failure PDFoxyc0n999Оценок пока нет
- 8 HutjensДокумент6 страниц8 HutjensHaris Nur MustofaОценок пока нет
- Bmi Asia PasifikДокумент4 страницыBmi Asia PasifikbxrbxrОценок пока нет
- Addison'sДокумент4 страницыAddison'sKoRnflakesОценок пока нет
- Supplement Reference Guide: 1 Edition 2009Документ234 страницыSupplement Reference Guide: 1 Edition 2009domОценок пока нет
- Nutrition Transition and Obesity Among Teenagers AДокумент3 страницыNutrition Transition and Obesity Among Teenagers AUthu DwifitriОценок пока нет
- Funny SpeechДокумент6 страницFunny SpeechMirza Naveed AkhtarОценок пока нет
- Surgical InfectionsДокумент54 страницыSurgical Infectionsmanish shresthaОценок пока нет
- The 8-Minute Workout - Men's HealthДокумент6 страницThe 8-Minute Workout - Men's HealthAboubakr JazairiОценок пока нет