Вам также может понравиться
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (120)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- As 3789.2-1991 Textiles For Health Care Facilities and Institutions Theatre Linen and Pre-PacksДокумент9 страницAs 3789.2-1991 Textiles For Health Care Facilities and Institutions Theatre Linen and Pre-PacksSAI Global - APACОценок пока нет
- q2 Long Quiz 002 EntreДокумент8 страницq2 Long Quiz 002 EntreMonn Justine Sabido0% (1)
- Paul S. Adler - Paul Du Gay - Glenn Morgan - Michael Reed (Eds.) - The Oxford Handbook of Sociology, Social Theory, and Organization Studies - Contemporary Currents-Oxford University Press, USA (2014)Документ817 страницPaul S. Adler - Paul Du Gay - Glenn Morgan - Michael Reed (Eds.) - The Oxford Handbook of Sociology, Social Theory, and Organization Studies - Contemporary Currents-Oxford University Press, USA (2014)Andreea Dobrita67% (3)
- Book Notes Covering: Andy Kirk's Book, Data Visualization - A Successful Design ProcessДокумент10 страницBook Notes Covering: Andy Kirk's Book, Data Visualization - A Successful Design ProcessDataVersed100% (1)
- Digitalisasi Alquran-1 PDFДокумент40 страницDigitalisasi Alquran-1 PDFMohammad Zildan Pasyha MОценок пока нет
- Kudla Vs PolandДокумент4 страницыKudla Vs PolandTony TopacioОценок пока нет
- ShinojДокумент4 страницыShinojArish BallanaОценок пока нет
- Rajkumar Kitchen Model Oil Expeller - INRДокумент1 страницаRajkumar Kitchen Model Oil Expeller - INRNishant0% (1)
- New VLSIДокумент2 страницыNew VLSIRanjit KumarОценок пока нет
- HP ELITEBOOK 8740W Inventec Armani 6050A2266501Документ61 страницаHP ELITEBOOK 8740W Inventec Armani 6050A2266501Gerardo Mediabilla0% (2)
- WTO & MFA AnalysisДокумент17 страницWTO & MFA Analysisarun1974Оценок пока нет
- On The Backward Problem For Parabolic Equations With MemoryДокумент19 страницOn The Backward Problem For Parabolic Equations With MemorykamranОценок пока нет
- Kolodin Agreement For Discipline by ConsentДокумент21 страницаKolodin Agreement For Discipline by ConsentJordan ConradsonОценок пока нет
- Claim Age Pension FormДокумент25 страницClaim Age Pension FormMark LordОценок пока нет
- Aircraft MaintenanceДокумент32 страницыAircraft MaintenanceTateОценок пока нет
- Lab 1Документ8 страницLab 1Нурболат ТаласбайОценок пока нет
- Lec05-Brute Force PDFДокумент55 страницLec05-Brute Force PDFHu D AОценок пока нет
- Psychological Attitude Towards SafetyДокумент17 страницPsychological Attitude Towards SafetyAMOL RASTOGI 19BCM0012Оценок пока нет
- NGOs in Satkhira PresentationДокумент17 страницNGOs in Satkhira PresentationRubayet KhundokerОценок пока нет
- IMS DB Interview Questions: Beginner LevelДокумент19 страницIMS DB Interview Questions: Beginner LevelsudhakarcheedaraОценок пока нет
- Hilti AnchorДокумент5 страницHilti AnchorGopi KrishnanОценок пока нет
- Hi 3 Yt 318201Документ3 страницыHi 3 Yt 318201partha khatuaОценок пока нет
- A Study On Impact of Smartphone AddictioДокумент4 страницыA Study On Impact of Smartphone AddictiotansuoragotОценок пока нет
- A-Panel Dual Polarization Half-Power Beam Width Adjust. Electr. DowntiltДокумент2 страницыA-Panel Dual Polarization Half-Power Beam Width Adjust. Electr. DowntiltUzair AkbarОценок пока нет
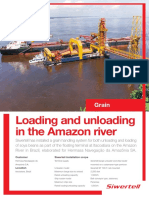
- Casesheet 086 Siwertell Hermasa Brazil Grain Unloader TerminalДокумент2 страницыCasesheet 086 Siwertell Hermasa Brazil Grain Unloader TerminalersОценок пока нет
- Note 2958296 Pre-Implementation Steps: Create Table TypeДокумент3 страницыNote 2958296 Pre-Implementation Steps: Create Table Typevishnu900890Оценок пока нет
- Asme Pvho-2-2019Документ61 страницаAsme Pvho-2-2019Vijay KumarОценок пока нет
- Joseph J. Fiumara v. Fireman's Fund Insurance Companies, 746 F.2d 87, 1st Cir. (1984)Документ7 страницJoseph J. Fiumara v. Fireman's Fund Insurance Companies, 746 F.2d 87, 1st Cir. (1984)Scribd Government DocsОценок пока нет
- Charts & Publications: Recommended Retail Prices (UK RRP)Документ3 страницыCharts & Publications: Recommended Retail Prices (UK RRP)KishanKashyapОценок пока нет
- Curriculum Vitae H R VijayДокумент8 страницCurriculum Vitae H R VijayvijaygowdabdvtОценок пока нет