Вам также может понравиться
- CBTAgustus 2020Документ154 страницыCBTAgustus 2020dokmi dmОценок пока нет
- Cardiac DysrhytmiasДокумент24 страницыCardiac DysrhytmiasAan KhaerismanОценок пока нет
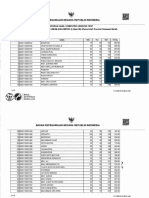
- Daftar Obat Puskesmes Banggae IДокумент3 страницыDaftar Obat Puskesmes Banggae IAan KhaerismanОценок пока нет
- Pengumuman Pemilihan Peminatan Ns Individual Periode X Tahun 2018 PDFДокумент3 страницыPengumuman Pemilihan Peminatan Ns Individual Periode X Tahun 2018 PDFAan KhaerismanОценок пока нет
- 1 Pembukaan - Basic Surgical SkillДокумент6 страниц1 Pembukaan - Basic Surgical SkillAan KhaerismanОценок пока нет
- Idhe 2009 London Malnutrition FennДокумент90 страницIdhe 2009 London Malnutrition FennAan KhaerismanОценок пока нет
- Judul MP WortelДокумент1 страницаJudul MP WortelAan KhaerismanОценок пока нет
- Sulbar Sesi 01 10 Nop 2018Документ6 страницSulbar Sesi 01 10 Nop 2018Aan KhaerismanОценок пока нет
- Volvulus of Small Bowel in A Case of Simple Meconium IleusДокумент3 страницыVolvulus of Small Bowel in A Case of Simple Meconium IleusMuhammad Bilal Mirza100% (1)
- U13 UE Amputations TFH EditsДокумент64 страницыU13 UE Amputations TFH EditsAan KhaerismanОценок пока нет
- Schizophrenia Fact SheetДокумент1 страницаSchizophrenia Fact SheetAan KhaerismanОценок пока нет
- 3 - Siklus Sel & Pembelahan SelДокумент23 страницы3 - Siklus Sel & Pembelahan SelAan KhaerismanОценок пока нет
- Dementia-Kuliah UMJ 07Документ18 страницDementia-Kuliah UMJ 07Aan KhaerismanОценок пока нет
- Heart Valve DiseaseДокумент9 страницHeart Valve DiseaseChaturangaNSenerathОценок пока нет
- 2 MorphologyДокумент43 страницы2 MorphologyAan KhaerismanОценок пока нет
- Case SharizalДокумент36 страницCase SharizalAan KhaerismanОценок пока нет
- Tibiofemoral alignment forces knee angles stresses cartilageДокумент12 страницTibiofemoral alignment forces knee angles stresses cartilageAan KhaerismanОценок пока нет
- Tibiofemoral alignment forces knee angles stresses cartilageДокумент12 страницTibiofemoral alignment forces knee angles stresses cartilageAan KhaerismanОценок пока нет
- 1 - Kuliah Pengenalan OrganДокумент155 страниц1 - Kuliah Pengenalan OrganAan KhaerismanОценок пока нет
- Hosts UmbrellaДокумент1 страницаHosts UmbrellaFabsor SoralОценок пока нет
- Finger TipДокумент11 страницFinger TipAan KhaerismanОценок пока нет
- Tibiofemoral alignment forces knee angles stresses cartilageДокумент12 страницTibiofemoral alignment forces knee angles stresses cartilageAan KhaerismanОценок пока нет
- Tibiofemoral alignment forces knee angles stresses cartilageДокумент12 страницTibiofemoral alignment forces knee angles stresses cartilageAan KhaerismanОценок пока нет
- Finger Tip Injury of The Right Index FingerДокумент32 страницыFinger Tip Injury of The Right Index FingerAan KhaerismanОценок пока нет
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- Lamaran - Produksi (Yusuf)Документ3 страницыLamaran - Produksi (Yusuf)Salatiga ParamedicОценок пока нет
- WW.05.21 Forceps Assisted Vaginal DeliveryДокумент3 страницыWW.05.21 Forceps Assisted Vaginal DeliveryLani Munawir Holis HolisОценок пока нет
- Autoimmune Encephalitis Syndromes With Antibodies - UpToDateДокумент1 страницаAutoimmune Encephalitis Syndromes With Antibodies - UpToDateSamОценок пока нет
- Anand Agrawal e CigДокумент4 страницыAnand Agrawal e CigAfianti SulastriОценок пока нет
- Ipls & AptsДокумент84 страницыIpls & AptsDesalegn TesfayeОценок пока нет
- 3-Day Food LogДокумент4 страницы3-Day Food LogiMangekyou30Оценок пока нет
- Course Outlinein PE 1 (PAFTHFit 1) MTC - SWДокумент4 страницыCourse Outlinein PE 1 (PAFTHFit 1) MTC - SWShaynerose HermogenoОценок пока нет
- Schwartz M. William. Pedoman Klinis Pediatri. Jakarta: Penerbit Buku Kedokteran. ECG. 2005Документ2 страницыSchwartz M. William. Pedoman Klinis Pediatri. Jakarta: Penerbit Buku Kedokteran. ECG. 2005Muhammad Rifky Ersadian NoorОценок пока нет
- Viral Exanthems and EnanthemsДокумент2 страницыViral Exanthems and Enanthemsclark146Оценок пока нет
- The Complex Relationship Between Diet and Health: Food Health: An OverviewДокумент8 страницThe Complex Relationship Between Diet and Health: Food Health: An OverviewNarayana Swaroop VeerubhotlaОценок пока нет
- Jaundice-Review of Clinical Features, Differential Diagnosis and RemediesДокумент13 страницJaundice-Review of Clinical Features, Differential Diagnosis and RemediesDr-Dalya ShakirОценок пока нет
- UN Millennium Development GoalДокумент1 страницаUN Millennium Development GoalEugene SmithОценок пока нет
- Oral Health Beyond Mouth: Patients' Opinions On Extraoral ExaminationДокумент6 страницOral Health Beyond Mouth: Patients' Opinions On Extraoral ExaminationAbbass El-OutaОценок пока нет
- Victoria Grigorita Resume 2015Документ2 страницыVictoria Grigorita Resume 2015api-283774863Оценок пока нет
- The Art of Taking A Medical HistoryДокумент4 страницыThe Art of Taking A Medical HistorypuneetОценок пока нет
- Mental Health L3 Workbook 1Документ116 страницMental Health L3 Workbook 1Nabeel MerchantОценок пока нет
- The Role of Physical Education in Promoting Healthy LifestylesДокумент42 страницыThe Role of Physical Education in Promoting Healthy Lifestylesjamessabraham2Оценок пока нет
- Bahasa Inggris MakalahДокумент6 страницBahasa Inggris MakalahtrisnaulandariОценок пока нет
- Internal Medicine Review: Key Concepts and Practice QuestionsДокумент26 страницInternal Medicine Review: Key Concepts and Practice QuestionsDivine SangutanОценок пока нет
- BP Environmental CleaningДокумент250 страницBP Environmental CleaningFaruque SathiОценок пока нет
- Supine Hypotensive Syndrome Signs, Causes and TreatmentДокумент6 страницSupine Hypotensive Syndrome Signs, Causes and TreatmentDimas RadityaОценок пока нет
- Zika virus knowledge and attitudesДокумент3 страницыZika virus knowledge and attitudesTeguh firmansyahОценок пока нет
- AZBESTДокумент2 страницыAZBESTgiska77Оценок пока нет
- Dr. Gideon KorenДокумент111 страницDr. Gideon KorenDINKER MAHAJANОценок пока нет
- Standart CostingДокумент13 страницStandart Costingboba milkОценок пока нет
- Live Guide Powerpoint v3Документ43 страницыLive Guide Powerpoint v3jonesОценок пока нет
- Pengaruh Kompres Dingin Terhadap Penurunan Nyeri Persalinan Kala I Pada Ibu Bersalin Di Wilayah Kerja Puskesmas Batu Aji Kota Batam TAHUN 2018Документ5 страницPengaruh Kompres Dingin Terhadap Penurunan Nyeri Persalinan Kala I Pada Ibu Bersalin Di Wilayah Kerja Puskesmas Batu Aji Kota Batam TAHUN 2018Arisa CaОценок пока нет
- 1.parotitis Practice Essentials, Pathophysiology, EpidemiologyДокумент12 страниц1.parotitis Practice Essentials, Pathophysiology, Epidemiologyandi elsa mulya pratiwiОценок пока нет
- Pearson Vue 1000 File (Corrected 11-2017)Документ245 страницPearson Vue 1000 File (Corrected 11-2017)adamОценок пока нет
- Brief History of Advocacy in Mental Health, The Roots of The Recovery MovementДокумент19 страницBrief History of Advocacy in Mental Health, The Roots of The Recovery MovementAndre BarkilОценок пока нет