Вам также может понравиться
- Perfume Formulation Technology Hand BookДокумент16 страницPerfume Formulation Technology Hand BookFaltumsg30% (10)
- Understanding and Completing The Reversion (25pp)Документ25 страницUnderstanding and Completing The Reversion (25pp)Tony Lambert100% (3)
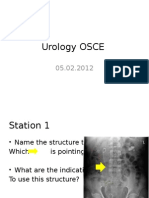
- Urology OSCEДокумент9 страницUrology OSCEJihad Anad75% (4)
- Urinary DiversionДокумент11 страницUrinary Diversionvlad910Оценок пока нет
- Aleister Crowley - The Book of The Law Cd4 Id1728400953 Size259Документ14 страницAleister Crowley - The Book of The Law Cd4 Id1728400953 Size259Jihad AnadОценок пока нет
- Manual of Urology - Diagnosis & Therapy (2nd Ed.)Документ362 страницыManual of Urology - Diagnosis & Therapy (2nd Ed.)Alina Ghe100% (3)
- PCNL and PyelolithotomyДокумент60 страницPCNL and PyelolithotomyDoctors PodcastОценок пока нет
- Nephro-Urology Monthly Nephro-Urology Monthly Nephro-Urology MonthlyДокумент3 страницыNephro-Urology Monthly Nephro-Urology Monthly Nephro-Urology MonthlyTheQueensafa90Оценок пока нет
- Karami 022 029Документ8 страницKarami 022 029TheQueensafa90Оценок пока нет
- Exploración Del ColédocoДокумент14 страницExploración Del ColédocoJavier VegaОценок пока нет
- 012011SCNA3Документ14 страниц012011SCNA3mariafmhОценок пока нет
- Buccal Mucosa Urethroplasty For Adult Urethral Strictures - PMCДокумент13 страницBuccal Mucosa Urethroplasty For Adult Urethral Strictures - PMCEllya Syahfitri 2108125983Оценок пока нет
- LaparoscopeДокумент9 страницLaparoscopedharmaОценок пока нет
- Percutaneous Nephrostomy: Last Updated: January 3, 2003Документ5 страницPercutaneous Nephrostomy: Last Updated: January 3, 2003Alicia EncinasОценок пока нет
- Drenaj EndoscopicДокумент20 страницDrenaj EndoscopicLivia GudacОценок пока нет
- Timetable PosterExДокумент45 страницTimetable PosterExNeo Rodriguez AlvaradoОценок пока нет
- Combined Laparoscopic Pyelolithotomy and Endoscopic Pyelolithotripsy For Staghorn Calculi: Long-Term Follow-Up Results From A Case SeriesДокумент6 страницCombined Laparoscopic Pyelolithotomy and Endoscopic Pyelolithotripsy For Staghorn Calculi: Long-Term Follow-Up Results From A Case SeriesantonОценок пока нет
- Adam 2017Документ4 страницыAdam 2017Bandac AlexandraОценок пока нет
- Sir 23205Документ4 страницыSir 23205ReyОценок пока нет
- Focus: Real-Time Ultrasound-Guided External Ventricular Drain Placement: Technical NoteДокумент5 страницFocus: Real-Time Ultrasound-Guided External Ventricular Drain Placement: Technical NoteOdiet RevenderОценок пока нет
- Retroperitoneal HeminephrectomyДокумент4 страницыRetroperitoneal HeminephrectomyIoannis ValioulisОценок пока нет
- FP & NC Kidney SurgeryДокумент48 страницFP & NC Kidney SurgeryancoursОценок пока нет
- Uretrostomia AtlasДокумент10 страницUretrostomia AtlasquirinalОценок пока нет
- Translate RadiologiДокумент1 страницаTranslate RadiologiAnonymous L3q7yHhhОценок пока нет
- Nephrectomy ProcedureДокумент4 страницыNephrectomy ProcedureRon Java FantillanОценок пока нет
- Assessment TN MasrukhiДокумент3 страницыAssessment TN MasrukhiAngger SatriaОценок пока нет
- Endoscopic Management of Complications From Laparoscopic Cholecystectomy - UpToDateДокумент16 страницEndoscopic Management of Complications From Laparoscopic Cholecystectomy - UpToDateLuis Miguel Díaz VegaОценок пока нет
- 1 s2.0 S2667008923000253 MainДокумент4 страницы1 s2.0 S2667008923000253 Mainal malikОценок пока нет
- Review StrikturДокумент13 страницReview StrikturFryda 'buona' YantiОценок пока нет
- Techniques of Vats LobectomyДокумент5 страницTechniques of Vats Lobectomyalexandra mendozaОценок пока нет
- Supine Percutaneous Nephrolithotomy in Horseshoe KidneyДокумент6 страницSupine Percutaneous Nephrolithotomy in Horseshoe KidneyDewi HenssaОценок пока нет
- Aaa RotoДокумент11 страницAaa RotoKarely TapiaОценок пока нет
- Management of Anastomotic Leaks After Esophagectomy and Gastric Pull-UpДокумент9 страницManagement of Anastomotic Leaks After Esophagectomy and Gastric Pull-UpSergio Sitta TarquiniОценок пока нет
- Editorial What Is The Best Endoscopic Treatment For Pancreatic PseudocystДокумент4 страницыEditorial What Is The Best Endoscopic Treatment For Pancreatic PseudocystLogical MonsterОценок пока нет
- Central Venous Catheter - StatPearls - NCBI BookshelfДокумент13 страницCentral Venous Catheter - StatPearls - NCBI Bookshelfrizki ahmad salehОценок пока нет
- How To Approach: Ureteral Obstructions in Dogs and CatsДокумент9 страницHow To Approach: Ureteral Obstructions in Dogs and Catsaniel_bmОценок пока нет
- B - Bile Duct Injuries in The Era of Laparoscopic Cholecystectomies - 2010Документ16 страницB - Bile Duct Injuries in The Era of Laparoscopic Cholecystectomies - 2010Battousaih1Оценок пока нет
- Diagnosis of A Strangulated Laparoscopic Incisional Hernia With Point-of-Care UltrasonographyДокумент3 страницыDiagnosis of A Strangulated Laparoscopic Incisional Hernia With Point-of-Care UltrasonographysaminОценок пока нет
- Yeyunos LaparosДокумент7 страницYeyunos LaparosFlipОценок пока нет
- Revisiting The Predictive Factors For Intra-Op-erative Complications of Rigid UreterosДокумент8 страницRevisiting The Predictive Factors For Intra-Op-erative Complications of Rigid UreterosTatik HandayaniОценок пока нет
- Vandenberg 2015Документ8 страницVandenberg 2015Zven BlackОценок пока нет
- ERCP Diagnostik Dan TerapeutikДокумент5 страницERCP Diagnostik Dan Terapeutikrisyda_mkhОценок пока нет
- Mini Percutaneous Nephrolithotomy in The Treatment ofДокумент8 страницMini Percutaneous Nephrolithotomy in The Treatment ofthanhtung1120002022Оценок пока нет
- A Simple Technique of Portal Vein Resection and Reconstruction During PancreaticoduodenectomyДокумент6 страницA Simple Technique of Portal Vein Resection and Reconstruction During Pancreaticoduodenectomyyacine26Оценок пока нет
- Ureteral Stent For Ureteral Stricture: James F. Borin and Elspeth M. McdougallДокумент13 страницUreteral Stent For Ureteral Stricture: James F. Borin and Elspeth M. McdougallOoОценок пока нет
- Nefrolitiasis RadiologiДокумент9 страницNefrolitiasis RadiologiSteven SetioОценок пока нет
- Muhammad Sajid Bin Mohd Rafee 112016389 DR Abraham Sp.UДокумент38 страницMuhammad Sajid Bin Mohd Rafee 112016389 DR Abraham Sp.Umau tauОценок пока нет
- Intech Percutaneous Nephrostomy 1Документ19 страницIntech Percutaneous Nephrostomy 1Zamzam IbrahimОценок пока нет
- Estenosis de Uretra Posterior2015Документ12 страницEstenosis de Uretra Posterior2015Salv L RomoОценок пока нет
- Semi-Rigid Ureteroscopy: Indications, Tips, and Tricks: Lily A. Whitehurst Bhaskar K. SomaniДокумент7 страницSemi-Rigid Ureteroscopy: Indications, Tips, and Tricks: Lily A. Whitehurst Bhaskar K. SomaniUmar FarooqОценок пока нет
- Endourology and Stone Diseases: Original ArticlesДокумент5 страницEndourology and Stone Diseases: Original ArticlesTatik HandayaniОценок пока нет
- Acs 03 02 183Документ9 страницAcs 03 02 183Evelin PetreОценок пока нет
- Knecht 1991Документ2 страницыKnecht 1991IHLIHLОценок пока нет
- Mainz II Surgery IllustratedДокумент25 страницMainz II Surgery IllustratedPurvi ParikhОценок пока нет
- Chapter 10 Sonographic Approach To Acute Abdominal PainДокумент13 страницChapter 10 Sonographic Approach To Acute Abdominal PainSyed Shahrul Naz SyedОценок пока нет
- Abdominoperineal Resection MilesДокумент17 страницAbdominoperineal Resection MilesHugoОценок пока нет
- Exploratory LaparotomyДокумент11 страницExploratory LaparotomyKris TejereroОценок пока нет
- Sotelo Et Al, Laparoscopic Rectovesical Fistula RepairДокумент5 страницSotelo Et Al, Laparoscopic Rectovesical Fistula RepairjordynixnОценок пока нет
- Endoscopic DacryocystorhinostomyДокумент17 страницEndoscopic Dacryocystorhinostomyapi-19500641Оценок пока нет
- Percutaneous Nephrolithotomy (PCNL)Документ8 страницPercutaneous Nephrolithotomy (PCNL)GERSON RYANTOОценок пока нет
- Content ServerДокумент12 страницContent ServerIrvan Dwi FitraОценок пока нет
- International Journal of Surgery Case ReportsДокумент4 страницыInternational Journal of Surgery Case Reportshussein_faourОценок пока нет
- Retrospective Study To Determine The Short-Term Outcomes of A Modified Pneumovesical Glenn-Anderson Procedure For Treating Primary Obstructing Megaureter. 2015Документ6 страницRetrospective Study To Determine The Short-Term Outcomes of A Modified Pneumovesical Glenn-Anderson Procedure For Treating Primary Obstructing Megaureter. 2015Paz MoncayoОценок пока нет
- Suprapubic Prostatectomy HinmanДокумент9 страницSuprapubic Prostatectomy HinmanputriОценок пока нет
- Percutaneous Surgery of the Upper Urinary Tract: Handbook of EndourologyОт EverandPercutaneous Surgery of the Upper Urinary Tract: Handbook of EndourologyPetrisor Aurelian GeavleteРейтинг: 5 из 5 звезд5/5 (1)
- Irrigating Fluids in Endoscopic Surgery: ReviewДокумент12 страницIrrigating Fluids in Endoscopic Surgery: ReviewJihad AnadОценок пока нет
- Gaur Et Al-2002-BJU InternationalДокумент5 страницGaur Et Al-2002-BJU InternationalJihad AnadОценок пока нет
- 4 5879809992000800192 PDFДокумент323 страницы4 5879809992000800192 PDFJihad AnadОценок пока нет
- WJCC 3 245Документ21 страницаWJCC 3 245Jihad AnadОценок пока нет
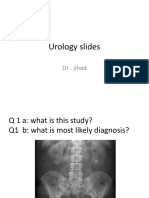
- Urology Slides: DR - JihadДокумент4 страницыUrology Slides: DR - JihadJihad Anad100% (1)
- Van de Graaff GeneratorДокумент10 страницVan de Graaff GeneratorJihad AnadОценок пока нет
- Uro SepsisДокумент23 страницыUro SepsisJihad Anad100% (1)
- Urethral BulkingДокумент7 страницUrethral BulkingJihad AnadОценок пока нет
- Kundalini Yoga & MeditationДокумент123 страницыKundalini Yoga & MeditationFejes Zoltan100% (4)
- Urology Slides: DR - JihadДокумент4 страницыUrology Slides: DR - JihadJihad Anad100% (1)
- Kundalini Yoga & MeditationДокумент123 страницыKundalini Yoga & MeditationFejes Zoltan100% (4)
- Git Contrast Study1Документ29 страницGit Contrast Study1Jihad AnadОценок пока нет
- CHA3545 Periurethral Bulking Agent PEДокумент10 страницCHA3545 Periurethral Bulking Agent PEJihad AnadОценок пока нет
- Hacking Made Easy by Dr. Robot and Hacking UniversityДокумент47 страницHacking Made Easy by Dr. Robot and Hacking UniversityJihad AnadОценок пока нет
- Ultrasound NotesДокумент19 страницUltrasound NotesJihad Anad100% (1)
- JSCFE Guidance Notes For Applicants - GenericДокумент2 страницыJSCFE Guidance Notes For Applicants - GenericJihad AnadОценок пока нет
- Ultrasound NotesДокумент19 страницUltrasound NotesJihad Anad100% (1)
- JSCFE Guidance Notes For Referees - GenericДокумент2 страницыJSCFE Guidance Notes For Referees - GenericJihad AnadОценок пока нет
- Answer For Urology MCQДокумент1 страницаAnswer For Urology MCQJihad AnadОценок пока нет
- Testicular TumoلبيrsДокумент58 страницTesticular TumoلبيrsJihad AnadОценок пока нет
- DiureticsДокумент6 страницDiureticsJihad AnadОценок пока нет
- Trauma Chapter 7 PDFДокумент22 страницыTrauma Chapter 7 PDFJihad AnadОценок пока нет
- Antibiotics: by Dr. Jihad AnadДокумент89 страницAntibiotics: by Dr. Jihad AnadJihad AnadОценок пока нет
- Penile Prosthesis Implantation in Chinese Patients With Severe Erectile Dysfunction: 10-Year ExperienceДокумент4 страницыPenile Prosthesis Implantation in Chinese Patients With Severe Erectile Dysfunction: 10-Year ExperienceJihad AnadОценок пока нет
- Penile Prosthes OutcomesДокумент42 страницыPenile Prosthes OutcomesJihad AnadОценок пока нет
- PCNL EeДокумент6 страницPCNL EeJihad AnadОценок пока нет
- Nursing Skills ChecklistДокумент8 страницNursing Skills Checklistapi-353656227Оценок пока нет
- Reasons For Managing Health and SafetyДокумент3 страницыReasons For Managing Health and SafetybrightОценок пока нет
- Foss L.-The End of Modern Medicine. Biomedical Science Under A Microscope-State Univ. of NY (2002) PDFДокумент352 страницыFoss L.-The End of Modern Medicine. Biomedical Science Under A Microscope-State Univ. of NY (2002) PDFSusi RutmalemОценок пока нет
- Indaegu: Exclusive Interview With Usain Bolt and His Agent, Ricky SimmsДокумент13 страницIndaegu: Exclusive Interview With Usain Bolt and His Agent, Ricky SimmsCraig WhiteОценок пока нет
- Questionnare On Work CultureДокумент6 страницQuestionnare On Work CultureManish RamnaniОценок пока нет
- Trends in Diagnosed Chronic Hepatitis B in A US Health System Population, 2006-2015Документ8 страницTrends in Diagnosed Chronic Hepatitis B in A US Health System Population, 2006-2015farid ahmadОценок пока нет
- 2020 Status Report As of August 31, 2021Документ192 страницы2020 Status Report As of August 31, 2021Jasper Kenneth PeraltaОценок пока нет
- S.N o Name of Drug Recommended Paediatrics Dose Strength 1.: CPM - 2 mg/5mlДокумент3 страницыS.N o Name of Drug Recommended Paediatrics Dose Strength 1.: CPM - 2 mg/5mlmrs raamОценок пока нет
- Road Safety EAL 338-1Документ53 страницыRoad Safety EAL 338-1NasrulОценок пока нет
- Safety Data Sheet: SECTION 1: Identification of The Substance/mixture and of The Company/undertakingДокумент11 страницSafety Data Sheet: SECTION 1: Identification of The Substance/mixture and of The Company/undertakingShahid BhattiОценок пока нет
- Progressive Addition Lens Design and The Short of Stature (Shan-Yu, S.)Документ3 страницыProgressive Addition Lens Design and The Short of Stature (Shan-Yu, S.)Valentina PereaОценок пока нет
- B.inggris Weny LestariДокумент5 страницB.inggris Weny LestariRatna SusantiОценок пока нет
- Iman Tavassoly CVДокумент6 страницIman Tavassoly CVGladis HutahaeanОценок пока нет
- Capnography Application in Acute and Critical Care: Tom Ahrens, DNS, RN, CCRN, CS Carrie Sona, MSN, RN, CCRN, CSДокумент10 страницCapnography Application in Acute and Critical Care: Tom Ahrens, DNS, RN, CCRN, CS Carrie Sona, MSN, RN, CCRN, CSJavier Enrique Barrera PachecoОценок пока нет
- 2021 A Guide To The African Human Rights System Celebrating 40 YearsДокумент115 страниц2021 A Guide To The African Human Rights System Celebrating 40 YearsChala Yuye KemerОценок пока нет
- Case Presentation: Hirsutism and OligomenorrheaДокумент20 страницCase Presentation: Hirsutism and Oligomenorrheadidu91Оценок пока нет
- Nursepreneurs Essay by J. BacarisasДокумент17 страницNursepreneurs Essay by J. BacarisasCris GalendezОценок пока нет
- Was King Tut Murdered?Документ4 страницыWas King Tut Murdered?mauricio760Оценок пока нет
- Nursing Care Plan 2 Knowledge DeficitДокумент7 страницNursing Care Plan 2 Knowledge Deficitdbryant0101100% (3)
- Panangbigbig Ken Panangisurat Kadagiti Numero Manipud 0 Aginggana 100Документ4 страницыPanangbigbig Ken Panangisurat Kadagiti Numero Manipud 0 Aginggana 100EVANGELINE DARRASОценок пока нет
- Development of Road Header Roof Bolting ModuleДокумент7 страницDevelopment of Road Header Roof Bolting ModuleCraig ThomasОценок пока нет
- Quantitative Analysis of Lead, Cadmium and Chromium Found in Selected Fish Marketed in Metro Manila, PhilippinesДокумент6 страницQuantitative Analysis of Lead, Cadmium and Chromium Found in Selected Fish Marketed in Metro Manila, PhilippinesMstkasrОценок пока нет
- "Nisi Dominus Frustra" College of Nursing & Allied Health Sciences Maasin City, Southern LeyteДокумент2 страницы"Nisi Dominus Frustra" College of Nursing & Allied Health Sciences Maasin City, Southern Leytecoosa liquorsОценок пока нет
- 6 - Tamplate For Incident - Accident - Near Miss ReportДокумент4 страницы6 - Tamplate For Incident - Accident - Near Miss ReportImran razaОценок пока нет
- Microbial Content and Diversity Inseveral Tempe From Bogor AreasДокумент9 страницMicrobial Content and Diversity Inseveral Tempe From Bogor AreasCendra KammiОценок пока нет
- Proposal For The BoosterДокумент5 страницProposal For The BoosterraziОценок пока нет
- Contractor Safety Management ProcessДокумент14 страницContractor Safety Management Processsrkam100% (2)
- Adverse Events Associated With Melatonin For The Treatment of Primary or Secondary Sleep Disorders: A Systematic ReviewДокумент20 страницAdverse Events Associated With Melatonin For The Treatment of Primary or Secondary Sleep Disorders: A Systematic ReviewZach Segmuel MiñanoОценок пока нет
- MalariaДокумент170 страницMalariatummalapalli venkateswara rao100% (4)