Вам также может понравиться
- Treatment of Acute Stress Disorder PDFДокумент4 страницыTreatment of Acute Stress Disorder PDFdreamingОценок пока нет
- Psychotherapy For Specific Phobia in Adults PDFДокумент6 страницPsychotherapy For Specific Phobia in Adults PDFdreamingОценок пока нет
- Psychotherapy For Obsessive-Compulsive Disorder PDFДокумент9 страницPsychotherapy For Obsessive-Compulsive Disorder PDFdreamingОценок пока нет
- Generalized Anxiety Disorder - Epidemiology, Pathogenesis, Clinical Manifestations, Course, Assessment, and Diagnosis PDFДокумент7 страницGeneralized Anxiety Disorder - Epidemiology, Pathogenesis, Clinical Manifestations, Course, Assessment, and Diagnosis PDFdreaming100% (1)
- Psychotherapy For Panic Disorder PDFДокумент9 страницPsychotherapy For Panic Disorder PDFdreaming100% (2)
- Pharmacotherapy For Social Anxiety Disorder PDFДокумент8 страницPharmacotherapy For Social Anxiety Disorder PDFdreamingОценок пока нет
- Pharmacotherapy For Panic Disorder PDFДокумент8 страницPharmacotherapy For Panic Disorder PDFdreamingОценок пока нет
- Co-Occurring Anxiety Disorders and Substance Use Disorders - Epidemiology, Clinical Manifestations, and Diagnosis PDFДокумент7 страницCo-Occurring Anxiety Disorders and Substance Use Disorders - Epidemiology, Clinical Manifestations, and Diagnosis PDFdreamingОценок пока нет
- Pharmacotherapy For Generalized Anxiety Disorder PDFДокумент16 страницPharmacotherapy For Generalized Anxiety Disorder PDFdreaming100% (1)
- Obsessive-Compulsive Disorder in Pregnant and Postpartum Women PDFДокумент6 страницObsessive-Compulsive Disorder in Pregnant and Postpartum Women PDFdreamingОценок пока нет
- Comorbid Anxiety and Depression - Epidemiology, Clinical Manifestations, and Diagnosis PDFДокумент24 страницыComorbid Anxiety and Depression - Epidemiology, Clinical Manifestations, and Diagnosis PDFdreaming0% (1)
- Obsessive-Compulsive Disorder in Adults - Epidemiology, Pathogenesis, Clinical Manifestations, Course, and Diagnosis PDFДокумент9 страницObsessive-Compulsive Disorder in Adults - Epidemiology, Pathogenesis, Clinical Manifestations, Course, and Diagnosis PDFdreamingОценок пока нет
- Pharmacotherapy For Specific Phobia in Adults PDFДокумент4 страницыPharmacotherapy For Specific Phobia in Adults PDFdreamingОценок пока нет
- Treatment of Acute Procedure Anxiety in Adults PDFДокумент7 страницTreatment of Acute Procedure Anxiety in Adults PDFdreaming100% (1)
- Combat Operational Stress Reaction PDFДокумент12 страницCombat Operational Stress Reaction PDFdreamingОценок пока нет
- Panic Disorder - Epidemiology, Pathogenesis, Clinical Manifestations, Course, Assessment, and Diagnosis PDFДокумент10 страницPanic Disorder - Epidemiology, Pathogenesis, Clinical Manifestations, Course, Assessment, and Diagnosis PDFdreamingОценок пока нет
- Agoraphobia in Adults - Epidemiology, Pathogenesis, Clinical Manifestations, Course, and Diagnosis PDFДокумент8 страницAgoraphobia in Adults - Epidemiology, Pathogenesis, Clinical Manifestations, Course, and Diagnosis PDFdreamingОценок пока нет
- Psychotherapy For Social Anxiety Disorder PDFДокумент6 страницPsychotherapy For Social Anxiety Disorder PDFdreaming100% (1)
- Psychotherapy For Generalized Anxiety Disorder PDFДокумент9 страницPsychotherapy For Generalized Anxiety Disorder PDFdreamingОценок пока нет
- Acute Stress Disorder - Epidemiology, Clinical Manifestations, and Diagnosis PDFДокумент6 страницAcute Stress Disorder - Epidemiology, Clinical Manifestations, and Diagnosis PDFdreaming100% (1)
- Acute Procedure Anxiety in Adults - Course, Screening, Assessment, and Differential Diagnosis PDFДокумент4 страницыAcute Procedure Anxiety in Adults - Course, Screening, Assessment, and Differential Diagnosis PDFdreamingОценок пока нет
- Posttraumatic Stress Disorder - Epidemiology, Pathophysiology, Clinical Manifestations, Course, and Diagnosis PDFДокумент10 страницPosttraumatic Stress Disorder - Epidemiology, Pathophysiology, Clinical Manifestations, Course, and Diagnosis PDFdreamingОценок пока нет
- Treatment For Specific Phobias of Medical and Dental Procedures PDFДокумент8 страницTreatment For Specific Phobias of Medical and Dental Procedures PDFdreamingОценок пока нет
- Deep Brain Stimulation For Treatment of Obsessive-Compulsive Disorder PDFДокумент6 страницDeep Brain Stimulation For Treatment of Obsessive-Compulsive Disorder PDFdreamingОценок пока нет
- Social Anxiety Disorder - Epidemiology, Clinical Manifestations, and Diagnosis PDFДокумент7 страницSocial Anxiety Disorder - Epidemiology, Clinical Manifestations, and Diagnosis PDFdreamingОценок пока нет
- Pharmacotherapy For Posttraumatic Stress Disorder PDFДокумент6 страницPharmacotherapy For Posttraumatic Stress Disorder PDFdreamingОценок пока нет
- Psychotherapy For Posttraumatic Stress Disorder PDFДокумент9 страницPsychotherapy For Posttraumatic Stress Disorder PDFdreamingОценок пока нет
- Treatment of Co-Occurring Anxiety Disorders and Substance Use Disorders PDFДокумент9 страницTreatment of Co-Occurring Anxiety Disorders and Substance Use Disorders PDFdreamingОценок пока нет
- Specific Phobia in Adults - Epidemiology, Clinical Manifestations, Course and Diagnosis PDFДокумент10 страницSpecific Phobia in Adults - Epidemiology, Clinical Manifestations, Course and Diagnosis PDFdreamingОценок пока нет
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (894)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- Effective Home Remedies With HerbsДокумент23 страницыEffective Home Remedies With HerbsAlexandru Vasile100% (1)
- The Teacher's Guide ToДокумент90 страницThe Teacher's Guide ToKellyn KlapaskaОценок пока нет
- CyclophosphamideДокумент3 страницыCyclophosphamideChen Boon TeyОценок пока нет
- Teva PharmaceuticalДокумент17 страницTeva PharmaceuticalGanesh VedhachalamОценок пока нет
- Syringe Pump ReportДокумент6 страницSyringe Pump ReportzulayieОценок пока нет
- Utility Validations - Review: Hvac Explain HVAC QualificationДокумент64 страницыUtility Validations - Review: Hvac Explain HVAC Qualifications lavanya100% (1)
- 6-Gingerol ArecolineДокумент8 страниц6-Gingerol Arecolineapi-327826901Оценок пока нет
- Various Drugs Used in Paediatric DentistryДокумент56 страницVarious Drugs Used in Paediatric DentistryPo PowОценок пока нет
- Quality Assurance,: A Systemic Approach For Effective ComplianceДокумент73 страницыQuality Assurance,: A Systemic Approach For Effective ComplianceHemanth PanasaОценок пока нет
- Royal Surgical April 2018 Outward Sales ReportДокумент6 страницRoyal Surgical April 2018 Outward Sales ReportManoj SharmaОценок пока нет
- Dissolution Testing of Poorly Soluble Compoundsolution TestingДокумент7 страницDissolution Testing of Poorly Soluble Compoundsolution TestingArranee ChotikoОценок пока нет
- Communication and Ethics in Pharmacy Practice: What Is To BeДокумент23 страницыCommunication and Ethics in Pharmacy Practice: What Is To BeMuhammad RezaОценок пока нет
- Brochure IIPRD 2012Документ6 страницBrochure IIPRD 2012satyadev_IIPRDОценок пока нет
- Zambia Health Shop GuidelinesДокумент18 страницZambia Health Shop Guidelinesdavies100% (1)
- Patient Medication Adherence PDFДокумент5 страницPatient Medication Adherence PDFAlexandrahautaОценок пока нет
- Poster PresentationДокумент1 страницаPoster PresentationsjОценок пока нет
- Puente PiedraДокумент6 страницPuente PiedraBotica Super FarmaОценок пока нет
- EtosuksimidДокумент14 страницEtosuksimidMaharani IndriatyОценок пока нет
- Receptors and PharmacodynamicsДокумент78 страницReceptors and PharmacodynamicsMuhammad Bilal Bin Amir100% (1)
- ECA Biological Raw Materials ExcipientsДокумент6 страницECA Biological Raw Materials ExcipientsBiopharma GuruОценок пока нет
- The High Cost of Prescription Drugs CausesДокумент5 страницThe High Cost of Prescription Drugs Causesjuddy avottОценок пока нет
- Hyoscine ButylbromideДокумент2 страницыHyoscine ButylbromideKepslock StahpОценок пока нет
- Group MembersДокумент28 страницGroup MembersBlackjack100% (1)
- Kiran Mazumdar ShawДокумент11 страницKiran Mazumdar ShawraghavmehraОценок пока нет
- Document (12) 1Документ7 страницDocument (12) 1Fazal JalalОценок пока нет
- PCP Regulations For Pharm.D ProgramДокумент21 страницаPCP Regulations For Pharm.D ProgramAdil YousafОценок пока нет
- DIS IPD Ceftriaxone KonsulДокумент28 страницDIS IPD Ceftriaxone KonsulTriana MaulidyahОценок пока нет
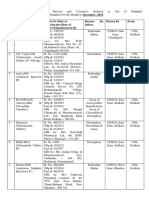
- Drug Alert For The Month of December 2016Документ3 страницыDrug Alert For The Month of December 2016amit545Оценок пока нет
- APEC Product Security Supply Chain Management SystemДокумент32 страницыAPEC Product Security Supply Chain Management SystemRenzo FernandezОценок пока нет
- Role of Echinocandins in Invasive Fungal InfectionsДокумент63 страницыRole of Echinocandins in Invasive Fungal Infectionsbanteng wibisonoОценок пока нет