Вам также может понравиться
- Monitoring The Progress of Labor: Marissa Villacarlos Nualla, MD, Fpogs, Fpsuog Mcu-College of MedicineДокумент58 страницMonitoring The Progress of Labor: Marissa Villacarlos Nualla, MD, Fpogs, Fpsuog Mcu-College of MedicineRozzie ReyesОценок пока нет
- Onechanbara - Bikini Samurai Squad Game GuideДокумент83 страницыOnechanbara - Bikini Samurai Squad Game GuideStefan RoscaОценок пока нет
- Catherine Davies - Modernity, Masculinity, and Imperfect Cinema in CubaДокумент16 страницCatherine Davies - Modernity, Masculinity, and Imperfect Cinema in CubakahlilchaarОценок пока нет
- Hematologic DiseasesДокумент11 страницHematologic DiseasesPerrilyn Perey100% (2)
- Din en 10346Документ45 страницDin en 10346Lucero AlemanОценок пока нет
- MalpresentationДокумент37 страницMalpresentationLovely SarangiОценок пока нет
- Chapter 1Документ38 страницChapter 1Kurt dela Torre100% (1)
- Complications in PregnancyДокумент81 страницаComplications in PregnancyTia TahniaОценок пока нет
- Nursing Care of The NewbornДокумент86 страницNursing Care of The Newbornjapzee1988100% (1)
- 3 (OB Cases)Документ267 страниц3 (OB Cases)Sharyl Plan SarominesОценок пока нет
- Placenta AccretaДокумент3 страницыPlacenta AccretaFigueroa John ReyОценок пока нет
- Essential Intrapartum and Newborn CareДокумент37 страницEssential Intrapartum and Newborn CareVenice s SantosОценок пока нет
- Hirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОт EverandHirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОценок пока нет
- Resume For Singapore Spass Civil EngineerДокумент8 страницResume For Singapore Spass Civil EngineerArul SD100% (1)
- NCM QuizДокумент7 страницNCM QuizKyla Marie NabongОценок пока нет
- Bubbles HeДокумент39 страницBubbles HePerrilyn PereyОценок пока нет
- Cesarean Section PatelДокумент55 страницCesarean Section Patelالوافي الذهبيОценок пока нет
- Of Gods, Glyphs and KingsДокумент24 страницыOf Gods, Glyphs and KingsBraulioОценок пока нет
- AutoPIPE Tutorial PDFДокумент156 страницAutoPIPE Tutorial PDFdhaktodesatyajitОценок пока нет
- Complications With The Passenger 2Документ77 страницComplications With The Passenger 2JudyОценок пока нет
- What Is The Difference?: EINC (Ma'am Nera Galan)Документ2 страницыWhat Is The Difference?: EINC (Ma'am Nera Galan)Angeline NavarroОценок пока нет
- Fractal Blaster Trading Strategy ReportДокумент22 страницыFractal Blaster Trading Strategy ReportIcky IckyОценок пока нет
- Placenta Previa and Abruptio Placenta: Presenter Eessaa ShresthaДокумент72 страницыPlacenta Previa and Abruptio Placenta: Presenter Eessaa ShresthaEsa SthaОценок пока нет
- Acute Renal FailureДокумент4 страницыAcute Renal FailurePerrilyn PereyОценок пока нет
- Normal and Abnormal Present IonДокумент31 страницаNormal and Abnormal Present IondeemОценок пока нет
- Forceps Delivery Treatment & Management - Preoperative Details, Intraoperative Details, Postoperative DetailsДокумент10 страницForceps Delivery Treatment & Management - Preoperative Details, Intraoperative Details, Postoperative DetailsAnonymous wYz8FtLLOОценок пока нет
- Fellowship 2nd Edition Book 2 - Inverse Fellowship (Playbooks)Документ44 страницыFellowship 2nd Edition Book 2 - Inverse Fellowship (Playbooks)AleОценок пока нет
- China Email ListДокумент3 страницыChina Email ListRosie Brown40% (5)
- High Risk PregnancyДокумент14 страницHigh Risk PregnancyJezrael PueblosОценок пока нет
- Essential Intrapartum Newborn CareДокумент36 страницEssential Intrapartum Newborn Carefatima chrystelle nuñal100% (1)
- My Kindergarten BookДокумент48 страницMy Kindergarten BookfranciscoОценок пока нет
- Bed Bath ExaMДокумент2 страницыBed Bath ExaMKweng Kweng DoongОценок пока нет
- Newborn Resuscitation ChecklistДокумент58 страницNewborn Resuscitation Checklistboinkjilijoy50% (2)
- Dystocia: DR - Selvaraj, Chinnasamy M.DДокумент54 страницыDystocia: DR - Selvaraj, Chinnasamy M.DSelvaraj ChinnasamyОценок пока нет
- MCH BulletsДокумент13 страницMCH BulletsPatziedawn GonzalvoОценок пока нет
- Placental Abnormalities Normal Placenta: © Mary Andrea G. Agorilla, Ust-Con 2021 - 1Документ3 страницыPlacental Abnormalities Normal Placenta: © Mary Andrea G. Agorilla, Ust-Con 2021 - 1Mary AgorillaОценок пока нет
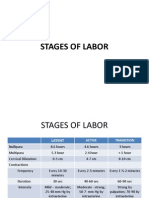
- Stages of LaborДокумент30 страницStages of LaborPerrilyn Perey100% (1)
- Nle - High-Risk PregnancyДокумент113 страницNle - High-Risk Pregnancytachycardia01Оценок пока нет
- L.obstetrics & Gynaecological NursingДокумент14 страницL.obstetrics & Gynaecological NursingAnjali Rahul AjmeriОценок пока нет
- High - Risk PregnancyДокумент110 страницHigh - Risk PregnancyAndre DityaОценок пока нет
- Abruptio Placenta and AbortionДокумент10 страницAbruptio Placenta and Abortiondanica grace gubaОценок пока нет
- Antepartum HaemorrhageДокумент74 страницыAntepartum HaemorrhageApex College of Nursing100% (1)
- Bleeding During PregnancyДокумент4 страницыBleeding During PregnancyCarl Andre ReyesОценок пока нет
- Prenatal Management (Part 4)Документ17 страницPrenatal Management (Part 4)Austine James Sabenicio PantiloОценок пока нет
- Breech DeliveryДокумент6 страницBreech DeliveryNyoman TapayanaОценок пока нет
- Cleansing Bed BathДокумент16 страницCleansing Bed BathRoger ViloОценок пока нет
- The Diagnosis of PregnancyДокумент76 страницThe Diagnosis of PregnancyCnette S. LumboОценок пока нет
- Curriculum in MalaysiaДокумент37 страницCurriculum in MalaysiaEmily Ling100% (1)
- Ps of LaborДокумент28 страницPs of LaborErvina Luisa Delias CampusОценок пока нет
- The Important Measurements of A NewbornДокумент3 страницыThe Important Measurements of A NewbornGraciaОценок пока нет
- Fetal DevelopmentДокумент35 страницFetal DevelopmentDjamnur AgnessiaОценок пока нет
- SituationdДокумент64 страницыSituationdIvory SantiagoОценок пока нет
- MalpresentationДокумент19 страницMalpresentationHanelie B. AldeaОценок пока нет
- Immediate Newborn CareДокумент21 страницаImmediate Newborn CareScarlet AmodiaОценок пока нет
- Introduction To Obstetrics & Midwifery CareДокумент18 страницIntroduction To Obstetrics & Midwifery CareWhirmey ChinyamaОценок пока нет
- Uterine ProlapseДокумент11 страницUterine ProlapseMelDred Cajes BolandoОценок пока нет
- Reva Rubin Maternal Role Attainment TheoryДокумент4 страницыReva Rubin Maternal Role Attainment TheoryLeonard LigutomОценок пока нет
- Intrapartum AssessmentДокумент22 страницыIntrapartum Assessmentanon_27233321950% (2)
- EpisiotomyДокумент49 страницEpisiotomyBharat ThapaОценок пока нет
- EclampsiaДокумент47 страницEclampsiarranindyaprabasaryОценок пока нет
- Postpartum Nursing PowerpointДокумент3 страницыPostpartum Nursing PowerpointAntonella VitaleОценок пока нет
- Signs of LaborДокумент5 страницSigns of Labormarianne_07Оценок пока нет
- SafeДокумент18 страницSafeSaripda JaramillaОценок пока нет
- Presentation 1Документ36 страницPresentation 1madhurima kunduОценок пока нет
- Perineal Genital Care PERFORMANCE-CHECKLISTДокумент2 страницыPerineal Genital Care PERFORMANCE-CHECKLISTMary joy PaaОценок пока нет
- Unit VIII PRESUMPTIVE SIGNS AND SYMPTOMS OF PREGNANCYДокумент5 страницUnit VIII PRESUMPTIVE SIGNS AND SYMPTOMS OF PREGNANCYNancy100% (1)
- Partograph Preparation and UseДокумент48 страницPartograph Preparation and Useannyeong_123100% (1)
- Introduction To Midwifery ObstetricДокумент1 страницаIntroduction To Midwifery Obstetricnursing schoolОценок пока нет
- Cord Care: By: Abella, Wenalyn Grace ZДокумент6 страницCord Care: By: Abella, Wenalyn Grace ZWenalyn Grace Abella Llavan100% (1)
- Maternal and Child Health NursingДокумент73 страницыMaternal and Child Health NursingEcquin CapzyОценок пока нет
- Perineal Care ProcedureДокумент12 страницPerineal Care ProcedureShikarin KitaОценок пока нет
- Maternal QuizДокумент3 страницыMaternal QuizJeffrey ViernesОценок пока нет
- FWPДокумент37 страницFWPhemaanandhyОценок пока нет
- 2-Checklist For Pelvis AssessmentДокумент3 страницы2-Checklist For Pelvis AssessmentGazala ParveenОценок пока нет
- Destructive OperationsДокумент24 страницыDestructive OperationsSecret AgentОценок пока нет
- Fanconi Anemia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОт EverandFanconi Anemia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОценок пока нет
- Excess Fluid Volume PPT (Case Press)Документ10 страницExcess Fluid Volume PPT (Case Press)Perrilyn PereyОценок пока нет
- LaminectomyДокумент6 страницLaminectomyPerrilyn Perey100% (1)
- Arrest of DescentДокумент5 страницArrest of DescentPerrilyn PereyОценок пока нет
- OR TermsДокумент1 страницаOR TermsPerrilyn PereyОценок пока нет
- Nihms281140.pdf BibliographyДокумент13 страницNihms281140.pdf BibliographyPerrilyn PereyОценок пока нет
- Critcare PDFДокумент20 страницCritcare PDFPerrilyn PereyОценок пока нет
- Leg or Foot Amputation Pref CardДокумент2 страницыLeg or Foot Amputation Pref CardPerrilyn PereyОценок пока нет
- Anxiety Related 2010Документ17 страницAnxiety Related 2010Perrilyn PereyОценок пока нет
- Drug NameДокумент1 страницаDrug NamePerrilyn PereyОценок пока нет
- MenstruationДокумент1 страницаMenstruationPerrilyn PereyОценок пока нет
- Health Assessment Form Scribd.Документ1 страницаHealth Assessment Form Scribd.Perrilyn PereyОценок пока нет
- STAS 111 - Information AgeДокумент20 страницSTAS 111 - Information AgeMayeee GayosoОценок пока нет
- Division of Genetics ICAR-Indian Agricultural Research Institute, New Delhi - 110012Документ9 страницDivision of Genetics ICAR-Indian Agricultural Research Institute, New Delhi - 110012Shivam PateriyaОценок пока нет
- PoGo GymDef Cheat SheetДокумент1 страницаPoGo GymDef Cheat SheetFerni Panchito VillaОценок пока нет
- Floline Size eДокумент4 страницыFloline Size eNikesh ShahОценок пока нет
- Material Safety Data Sheet: Manufacturer Pt. Bital AsiaДокумент3 страницыMaterial Safety Data Sheet: Manufacturer Pt. Bital AsiaediОценок пока нет
- Architecture As Interface - Healing Architecture For Epatients. In: Healing Architecture. Hrsg. Nickl-Weller. 2013Документ6 страницArchitecture As Interface - Healing Architecture For Epatients. In: Healing Architecture. Hrsg. Nickl-Weller. 2013Asmaa AyadОценок пока нет
- Apy1 Kinematics Review - 2015 - KeyДокумент13 страницApy1 Kinematics Review - 2015 - KeyemadОценок пока нет
- Theological Differences Between Christianity and IslamДокумент18 страницTheological Differences Between Christianity and IslamMencari KhadijahОценок пока нет
- Sample Invoice PDFДокумент3 страницыSample Invoice PDFMarcus OlivieraaОценок пока нет
- The Brain in Your Pocket Evidence - That - SДокумент8 страницThe Brain in Your Pocket Evidence - That - Sanwaarft123Оценок пока нет
- Nocturne 2024Документ162 страницыNocturne 2024Peter JonesОценок пока нет
- HCT Baniqued P.D.E. Paper1 Version3 FullpaperДокумент8 страницHCT Baniqued P.D.E. Paper1 Version3 FullpaperJoshua HernandezОценок пока нет
- 70 Ijgm AsterДокумент12 страниц70 Ijgm AsterMc ManjuОценок пока нет
- Catalogue Mega EnglishДокумент40 страницCatalogue Mega EnglishInotech Outillage Nouvelle CalédonieОценок пока нет
- Optical CamouflageДокумент27 страницOptical CamouflageAlliluddin ShaikОценок пока нет
- Accounting For Financial Institutions Week 1Документ4 страницыAccounting For Financial Institutions Week 1emadhamdy2002Оценок пока нет
- 2016 Lesson 9Документ34 страницы2016 Lesson 9Junas Jr LaputОценок пока нет
- Determining The Value of The Acceleration Due To Gravity: President Ramon Magsaysay State UniversityДокумент12 страницDetermining The Value of The Acceleration Due To Gravity: President Ramon Magsaysay State UniversityKristian Anthony BautistaОценок пока нет