Вам также может понравиться
- Open Reduction and Internal Fixation (Orif) : Whatisitandwhydoineedit?Документ2 страницыOpen Reduction and Internal Fixation (Orif) : Whatisitandwhydoineedit?Asri Puji LestariОценок пока нет
- Pattern of Cutaneous Tuberculosis Among Children and AdolescentДокумент4 страницыPattern of Cutaneous Tuberculosis Among Children and AdolescentRamadhan Ananda PutraОценок пока нет
- 58TONEUJДокумент7 страниц58TONEUJRamadhan Ananda PutraОценок пока нет
- Tuberculosis of The SkinДокумент6 страницTuberculosis of The SkinRamadhan Ananda PutraОценок пока нет
- Treatment of CutaneousДокумент6 страницTreatment of CutaneousRamadhan Ananda PutraОценок пока нет
- Treatment of CutaneousДокумент6 страницTreatment of CutaneousRamadhan Ananda PutraОценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5782)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- Transcript of The Conversation With Henry KissingerДокумент24 страницыTranscript of The Conversation With Henry KissingerJeyannathann KarunanithiОценок пока нет
- wch13 01 Que 20230120Документ16 страницwch13 01 Que 20230120Rohee TariqОценок пока нет
- GB 1220 英文版Документ31 страницаGB 1220 英文版vasotermiОценок пока нет
- Spare Part List: Marine FCF Classic Series - 115V (60Hz) - 230V (50/60Hz) 12,000 - 16,000 BTU R410Документ4 страницыSpare Part List: Marine FCF Classic Series - 115V (60Hz) - 230V (50/60Hz) 12,000 - 16,000 BTU R410Hernando Fang PedrozaОценок пока нет
- Gradeup's comprehensive guide to teaching and learningДокумент6 страницGradeup's comprehensive guide to teaching and learningRJОценок пока нет
- Six Sigma ProjectДокумент77 страницSix Sigma ProjectSudhir Kumar100% (8)
- Acute Heart Failure in A 39-Year-Old ManДокумент2 страницыAcute Heart Failure in A 39-Year-Old Manhossein kasiriОценок пока нет
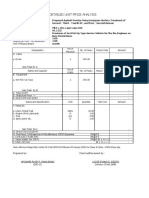
- DETAILED UNIT PRICE ANALYSIS FOR PROPOSED ASPHALT OVERLAYДокумент7 страницDETAILED UNIT PRICE ANALYSIS FOR PROPOSED ASPHALT OVERLAYreynoldОценок пока нет
- Bhimrao Ramji Ambedkar (: (Bimrawramdi Ambe KƏR) ʑ Ɽ ʱ Anthropologist OratorДокумент1 страницаBhimrao Ramji Ambedkar (: (Bimrawramdi Ambe KƏR) ʑ Ɽ ʱ Anthropologist OratorDevashish ChakrabartyОценок пока нет
- Present Perfect To PrintДокумент14 страницPresent Perfect To PrintLukas Art LM100% (1)
- A2B1 Unit 10bДокумент2 страницыA2B1 Unit 10bNguyễn VũОценок пока нет
- Icici PrudentialДокумент141 страницаIcici PrudentialBura NareshОценок пока нет
- IMC Sec-A Group-4 evaluates Mountain Dew ad conceptsДокумент3 страницыIMC Sec-A Group-4 evaluates Mountain Dew ad conceptsshibaniniОценок пока нет
- The Rime of The Ancient Mariner (Text of 1834) by - Poetry FoundationДокумент19 страницThe Rime of The Ancient Mariner (Text of 1834) by - Poetry FoundationNeil RudraОценок пока нет
- 4 3 3 1-Materials-Testing-LabДокумент7 страниц4 3 3 1-Materials-Testing-LabUday ChanОценок пока нет
- Savant Class v4.5.0Документ9 страницSavant Class v4.5.0Nameless0% (1)
- 4 362141008059695926Документ271 страница4 362141008059695926ze costaОценок пока нет
- Energy Transformations in Photosynthesis and RespirationДокумент8 страницEnergy Transformations in Photosynthesis and RespirationLyka Mae BenitoОценок пока нет
- Digitalcommons@University of Nebraska - Lincoln Digitalcommons@University of Nebraska - LincolnДокумент71 страницаDigitalcommons@University of Nebraska - Lincoln Digitalcommons@University of Nebraska - Lincolnเจฟ เรОценок пока нет
- Hirakud DamДокумент12 страницHirakud DamRmaryPandeyОценок пока нет
- Should Pornography Be BannedДокумент5 страницShould Pornography Be BannedVin VinОценок пока нет
- Mechatronics - Unit-Iii (Iv B.Tech I Sem Mech) : (Hydraulic Systems)Документ36 страницMechatronics - Unit-Iii (Iv B.Tech I Sem Mech) : (Hydraulic Systems)Radha KrishnaОценок пока нет
- ANSI/AWS D14.5-97 Specification For Welding of Presses and Press ComponentsДокумент157 страницANSI/AWS D14.5-97 Specification For Welding of Presses and Press Componentslightjp1Оценок пока нет
- Stock in Transit (GR - IR Regrouping - Reclassification) - SAP BlogsДокумент7 страницStock in Transit (GR - IR Regrouping - Reclassification) - SAP BlogsusamaОценок пока нет
- Year CompassДокумент10 страницYear CompassmeganОценок пока нет
- Galloway OPRA Request FormДокумент5 страницGalloway OPRA Request FormThe Citizens CampaignОценок пока нет
- Importance of AssessmenДокумент5 страницImportance of AssessmenFfffОценок пока нет
- Effectiveness of Free TrialsДокумент2 страницыEffectiveness of Free TrialstheoОценок пока нет
- Rephraring Exercises Key RepasoДокумент3 страницыRephraring Exercises Key RepasoAnonymous Lw1e6SmivОценок пока нет
- Syllabus TMG 1-0 EASAДокумент30 страницSyllabus TMG 1-0 EASAMarc RothОценок пока нет