Вам также может понравиться
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (894)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Teaching Plan - DIABETIC DIETДокумент9 страницTeaching Plan - DIABETIC DIETMarion Liana Dayrit67% (3)
- Todorov The Notion of LiteratureДокумент15 страницTodorov The Notion of LiteratureSiddhartha PratapaОценок пока нет
- Samples English Lessons Through LiteratureДокумент233 страницыSamples English Lessons Through LiteratureEmil Kosztelnik100% (1)
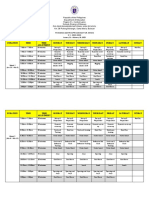
- Arnis Traning Matrix 2023Документ6 страницArnis Traning Matrix 2023RA CastroОценок пока нет
- Movers Speaking Test OverviewДокумент57 страницMovers Speaking Test OverviewThu HợpОценок пока нет
- Clinical Training Profile:: PhysiotherapyДокумент17 страницClinical Training Profile:: Physiotherapyrenata miateliОценок пока нет
- Insight Upper Intermediate International Answer KeyДокумент5 страницInsight Upper Intermediate International Answer KeySuzan Ibolari52% (31)
- Pain Management Teaching PlanДокумент9 страницPain Management Teaching PlanMarion Liana DayritОценок пока нет
- Goiter Teaching PlanДокумент5 страницGoiter Teaching PlanMarion Liana Dayrit100% (1)
- 00 B1 Practice Test 1 IntroductionДокумент6 страниц00 B1 Practice Test 1 IntroductionsalvaОценок пока нет
- DOH ANNUAL CALENDARДокумент3 страницыDOH ANNUAL CALENDARMarion Liana DayritОценок пока нет
- Narrative Report On The Division SeminarДокумент3 страницыNarrative Report On The Division Seminarvincevillamora2k11Оценок пока нет
- DrugsДокумент3 страницыDrugsMarion Liana DayritОценок пока нет
- Nutrition Guidelines To Improve Wound HealingДокумент8 страницNutrition Guidelines To Improve Wound HealingMarion Liana DayritОценок пока нет
- Fande Assignment: Saint Louis University School of NursingДокумент6 страницFande Assignment: Saint Louis University School of NursingMarion Liana DayritОценок пока нет
- PalliativeДокумент9 страницPalliativeMarion Liana DayritОценок пока нет
- Impaired Spontaneous VentilationДокумент1 страницаImpaired Spontaneous VentilationMarion Liana DayritОценок пока нет
- Patho PhysiologyДокумент5 страницPatho PhysiologyMarion Liana DayritОценок пока нет
- MalnutДокумент2 страницыMalnutMarion Liana DayritОценок пока нет
- ImmunizationsДокумент5 страницImmunizationsMarion Liana DayritОценок пока нет
- Interventions ArticleДокумент7 страницInterventions ArticleGary KartchnerОценок пока нет
- Accessscopingexercise ReportДокумент142 страницыAccessscopingexercise ReportMarion Liana DayritОценок пока нет
- 1459 Full PDFДокумент7 страниц1459 Full PDFMarion Liana DayritОценок пока нет
- Alterations in Elimination: GI Elimination Urinary EliminationДокумент27 страницAlterations in Elimination: GI Elimination Urinary EliminationMarion Liana DayritОценок пока нет
- Research Paper Template For CollegeДокумент4 страницыResearch Paper Template For Collegec9k7jjfk100% (1)
- Machiavelli 1Документ43 страницыMachiavelli 1api-295869438Оценок пока нет
- A101p1102141133D111030149雙語辭彙對照表Документ91 страницаA101p1102141133D111030149雙語辭彙對照表Albert LinОценок пока нет
- Foundations of Government Management: Muddling Through IncrementallyДокумент4 страницыFoundations of Government Management: Muddling Through IncrementallyAllan Viernes100% (1)
- Arun &associatesДокумент12 страницArun &associatesSujaa SaravanakhumaarОценок пока нет
- Mobile: 6303779851: CH - VasaviДокумент2 страницыMobile: 6303779851: CH - VasaviOmprakashОценок пока нет
- Investment Strategies and Portfolio ManagementДокумент9 страницInvestment Strategies and Portfolio ManagementRubi ZimmermanОценок пока нет
- Employee Development BrochureДокумент2 страницыEmployee Development Brochuredara moralezОценок пока нет
- ResearchДокумент37 страницResearchNadine LumanogОценок пока нет
- Final Professional M.B.B.S. Examination of July 2021: Select Student TypeДокумент4 страницыFinal Professional M.B.B.S. Examination of July 2021: Select Student Typeasif hossainОценок пока нет
- Reinabelle Reyes (Batch 2001) Reinabelle Reyes (Batch 2001) : The Life of Rodel Lasco, PHD (Batch 1977)Документ2 страницыReinabelle Reyes (Batch 2001) Reinabelle Reyes (Batch 2001) : The Life of Rodel Lasco, PHD (Batch 1977)Rivera MaeОценок пока нет
- Primera Lengua Extranjera II - Inglés Examen ResueltoДокумент4 страницыPrimera Lengua Extranjera II - Inglés Examen ResueltoAlbaОценок пока нет
- DiversityДокумент3 страницыDiversityapi-464306934Оценок пока нет
- Lesson 14Документ16 страницLesson 14Khmer Music100% (1)
- Blood Relationship As A Basis of Inheritance Under Islamic Law A Case Study of The Inner and Outer Circles of FamilyДокумент206 страницBlood Relationship As A Basis of Inheritance Under Islamic Law A Case Study of The Inner and Outer Circles of Familyisaac_naseerОценок пока нет
- Problems Encountered by Teachers in The Teaching-Learning Process: A Basis of An Action PlanДокумент20 страницProblems Encountered by Teachers in The Teaching-Learning Process: A Basis of An Action PlanERIKA O. FADEROGAOОценок пока нет
- Vanessa JoyДокумент23 страницыVanessa JoyAstigBermudezОценок пока нет
- Email@:: M.Harini +91-9487293806 +91-7305298360Документ2 страницыEmail@:: M.Harini +91-9487293806 +91-7305298360Praveen MalavaeОценок пока нет
- Artificial Intelligence Applications in Civil EngineeringДокумент31 страницаArtificial Intelligence Applications in Civil Engineeringpuppyarav2726Оценок пока нет
- Cpts 440 / 540 Artificial IntelligenceДокумент65 страницCpts 440 / 540 Artificial IntelligenceDuc Minh LeОценок пока нет
- Performance Appraisal AdvantagesДокумент6 страницPerformance Appraisal AdvantagesAnna HudsonОценок пока нет
- 15 March Daily Lesson PlanДокумент2 страницы15 March Daily Lesson PlanmocchiОценок пока нет