Вам также может понравиться
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Facs ProtocolДокумент7 страницFacs ProtocolmisterxОценок пока нет
- BT 2019Документ13 страницBT 2019biotech_vidhyaОценок пока нет
- Stripping For ReprobingДокумент2 страницыStripping For ReprobingStella SalvatoreОценок пока нет
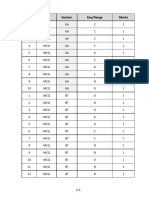
- Q.No. Type Section Key/Range MarksДокумент3 страницыQ.No. Type Section Key/Range Marksbiotech_vidhyaОценок пока нет
- Stripping For ReprobingДокумент2 страницыStripping For ReprobingStella SalvatoreОценок пока нет
- Polymerase Chain Reaction (PCR)Документ3 страницыPolymerase Chain Reaction (PCR)biotech_vidhyaОценок пока нет
- Brad FordДокумент12 страницBrad FordQi ChaoОценок пока нет
- SDS PageДокумент2 страницыSDS Pagebiotech_vidhyaОценок пока нет
- Buffer Preparation Guide for DNA/Protein Work (Shi LabДокумент6 страницBuffer Preparation Guide for DNA/Protein Work (Shi Labbiotech_vidhyaОценок пока нет
- Troubleshooting SDS-PAGE 1Документ3 страницыTroubleshooting SDS-PAGE 1biotech_vidhyaОценок пока нет
- Polymerasen GuideДокумент16 страницPolymerasen Guidebiotech_vidhyaОценок пока нет
- Components Reaction MixtureДокумент3 страницыComponents Reaction Mixturebiotech_vidhyaОценок пока нет
- Buffer Preparation Guide for DNA/Protein Work (Shi LabДокумент6 страницBuffer Preparation Guide for DNA/Protein Work (Shi Labbiotech_vidhyaОценок пока нет
- TNPSC Group 1 Prelim Book List PDFДокумент2 страницыTNPSC Group 1 Prelim Book List PDFbiotech_vidhyaОценок пока нет
- Whole Cell ExtractДокумент1 страницаWhole Cell Extractbiotech_vidhyaОценок пока нет
- TNPSC Group 1 Prelim Book List PDFДокумент2 страницыTNPSC Group 1 Prelim Book List PDFbiotech_vidhyaОценок пока нет
- Befcv List PDFДокумент22 страницыBefcv List PDFbiotech_vidhyaОценок пока нет
- Nuclear ExtractsДокумент2 страницыNuclear Extractsbiotech_vidhyaОценок пока нет
- Qpaper PondyДокумент21 страницаQpaper Pondybiotech_vidhyaОценок пока нет
- Ies 17 Set A Me Q AДокумент67 страницIes 17 Set A Me Q Abiotech_vidhyaОценок пока нет
- TNPSC Group 1 Prelim Book List PDFДокумент2 страницыTNPSC Group 1 Prelim Book List PDFbiotech_vidhyaОценок пока нет
- A.E. (Mechanical Engineering I) 2007Документ24 страницыA.E. (Mechanical Engineering I) 2007Mukesh KumarОценок пока нет
- Qpaper PondyДокумент21 страницаQpaper Pondybiotech_vidhyaОценок пока нет
- ESE 2017 Mechanical Engineering Prelims Exam Detailed SolutionДокумент52 страницыESE 2017 Mechanical Engineering Prelims Exam Detailed SolutionpataОценок пока нет
- Img Word-To PDFДокумент3 страницыImg Word-To PDFbiotech_vidhyaОценок пока нет
- Mechanical Engineering Code No. 14: Combined Competitive (Preliminary) Examination, 2010Документ20 страницMechanical Engineering Code No. 14: Combined Competitive (Preliminary) Examination, 2010biotech_vidhyaОценок пока нет
- TDC 41597 A (Mechanical Engg.) - 2012Документ20 страницTDC 41597 A (Mechanical Engg.) - 2012biotech_vidhyaОценок пока нет
- Recruitment RulesДокумент5 страницRecruitment Rulesbiotech_vidhyaОценок пока нет
- Part and Mold Design GuideДокумент170 страницPart and Mold Design GuideminhtintinОценок пока нет
- 1 TolerancesДокумент1 страница1 Tolerancesbiotech_vidhyaОценок пока нет
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (890)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- Geriatrics: Roger E. ThomasДокумент44 страницыGeriatrics: Roger E. ThomasSubhash SharmaОценок пока нет
- Malaysia PRP Private Hospital LogbookДокумент229 страницMalaysia PRP Private Hospital LogbookAiWeiОценок пока нет
- Personal Details and Training Log for Provisionally Registered PharmacistsДокумент48 страницPersonal Details and Training Log for Provisionally Registered PharmacistsB024-MASWANIE SOFEAОценок пока нет
- Geriatric Giants - DR SeymourДокумент108 страницGeriatric Giants - DR SeymourSharon Mallia100% (1)
- Health LiteracyДокумент5 страницHealth LiteracyHillary JamesОценок пока нет
- Dr. Dewi-Geriatric PharmacologyДокумент41 страницаDr. Dewi-Geriatric PharmacologyAnne Gustriwati0% (1)
- Best Practice Skin TearsДокумент25 страницBest Practice Skin TearsJacinta MontesОценок пока нет
- Too Many Pills - How Too Much Me - James Le FanuДокумент274 страницыToo Many Pills - How Too Much Me - James Le Fanumohamed gaberОценок пока нет
- Assessment of Rational Drug Use at Nagelle Arsi Veterinary Clinic West Arsi, Oromia, EthiopiaДокумент51 страницаAssessment of Rational Drug Use at Nagelle Arsi Veterinary Clinic West Arsi, Oromia, EthiopiaTamirat WakoОценок пока нет
- Ranitidine + OndansetronДокумент7 страницRanitidine + OndansetronAllicia PutriОценок пока нет
- Geri Assess Tools ArticleДокумент9 страницGeri Assess Tools ArticleThesmith FamОценок пока нет
- The Origin and Nature of Sorcery-Pharmakeia-Pharmaceutical ExplainedДокумент40 страницThe Origin and Nature of Sorcery-Pharmakeia-Pharmaceutical ExplainedArnulfo Yu LanibaОценок пока нет
- Test Bank For Ebersole and Hess Toward Healthy Aging 8th Edition Theris A TouhyДокумент8 страницTest Bank For Ebersole and Hess Toward Healthy Aging 8th Edition Theris A TouhyGraceLopezyfmox100% (31)
- Rapid Geriatric Assessment of Hip FractureДокумент14 страницRapid Geriatric Assessment of Hip FractureJuliana Moreno LadinoОценок пока нет
- Ageing Prisoners: An Introduction To Geriatric Health-Care Challenges in Correctional FacilitiesДокумент24 страницыAgeing Prisoners: An Introduction To Geriatric Health-Care Challenges in Correctional FacilitiesepraetorianОценок пока нет
- 2014 Geriatric Emergency Department GuidelinesДокумент19 страниц2014 Geriatric Emergency Department GuidelinesjujucastellОценок пока нет
- Fall Prevention: How Can Older Adults Prevent Falls?Документ4 страницыFall Prevention: How Can Older Adults Prevent Falls?Amalina ZahariОценок пока нет
- Pharmaceutical Care PDFДокумент18 страницPharmaceutical Care PDFAhmed IsseОценок пока нет
- NCM 113 EVIDENCE-BASED GERONTOLOGICAL NURSINGДокумент11 страницNCM 113 EVIDENCE-BASED GERONTOLOGICAL NURSINGAisha CorobongОценок пока нет
- GERIA Unit 4 LearnersДокумент34 страницыGERIA Unit 4 Learners3D - AURELIO, Lyca Mae M.Оценок пока нет
- New Approach For CV Risk Management (Prof. DR - Dr. Djanggan Sargowo, SPPD, SPJP (K) )Документ56 страницNew Approach For CV Risk Management (Prof. DR - Dr. Djanggan Sargowo, SPPD, SPJP (K) )Yulia SumarnaОценок пока нет
- Effect of Pharmacy Intervention To Patient With Polypharmacy - JournalДокумент7 страницEffect of Pharmacy Intervention To Patient With Polypharmacy - Journalanon_529380518Оценок пока нет
- StoppFrail PaperДокумент8 страницStoppFrail PaperEric LiangОценок пока нет
- Chapter 003 Geriatric Pharmacology: Multiple Choice QuestionsДокумент15 страницChapter 003 Geriatric Pharmacology: Multiple Choice QuestionsgoldfishxОценок пока нет
- Pharmacology and The Nursing Process 7th Edition Lilley Test BankДокумент25 страницPharmacology and The Nursing Process 7th Edition Lilley Test BankStevenCookexjrp100% (40)
- Polypharmacy in the elderlyДокумент3 страницыPolypharmacy in the elderlyjosephОценок пока нет
- Common Drug Side Effects - Drug Interactions - Elderly - Primary Care - 2017Документ8 страницCommon Drug Side Effects - Drug Interactions - Elderly - Primary Care - 2017opulgarОценок пока нет
- Exploring The Pharmaco-Clinical View On Bhanga (Cannabis Sativa Linn.) : A Classical Unfamiliar PortrayalДокумент20 страницExploring The Pharmaco-Clinical View On Bhanga (Cannabis Sativa Linn.) : A Classical Unfamiliar PortrayalVikram DravidОценок пока нет
- Adr Management and MonitoringДокумент5 страницAdr Management and MonitoringRaju NiraulaОценок пока нет
- Top-Rate Geriatric Care at Grace Nursing HomeДокумент11 страницTop-Rate Geriatric Care at Grace Nursing HomeRolli SptОценок пока нет