Вам также может понравиться
- Aircraft System Safety: Assessments for Initial Airworthiness CertificationОт EverandAircraft System Safety: Assessments for Initial Airworthiness CertificationОценок пока нет
- Application of Probabilistic Methods for the Safety Assessment and the Reliable Operation of Research ReactorsОт EverandApplication of Probabilistic Methods for the Safety Assessment and the Reliable Operation of Research ReactorsОценок пока нет
- RiskAnal Perspective-Jun04Документ7 страницRiskAnal Perspective-Jun04Panchdev KumarОценок пока нет
- Apostolakis 2004Документ6 страницApostolakis 2004Lorena CCОценок пока нет
- What Is A Qra and What Can It Tell You?: QuestДокумент9 страницWhat Is A Qra and What Can It Tell You?: QuesthazopmanОценок пока нет
- Ga TauДокумент15 страницGa Taufaisal canОценок пока нет
- Improve Process Safety With Near-Miss Analysis: On The HorizonДокумент8 страницImprove Process Safety With Near-Miss Analysis: On The HorizonUsama NiaziОценок пока нет
- Preliminary Hazard AnalysisДокумент4 страницыPreliminary Hazard AnalysisEdmundo PulidoОценок пока нет
- Safety, Reliability, Risk Management and Human Factors: An Integrated Engineering Approach Applied To Nuclear FacilitiesДокумент12 страницSafety, Reliability, Risk Management and Human Factors: An Integrated Engineering Approach Applied To Nuclear FacilitiesSouHeyb DaciОценок пока нет
- A Method For Barrier-Based Incident InvestigationДокумент7 страницA Method For Barrier-Based Incident InvestigationEzatollah SalaryОценок пока нет
- Human Error Chap 8 (James Reason)Документ44 страницыHuman Error Chap 8 (James Reason)Nasir DanialОценок пока нет
- Fault Tree AnalysisДокумент8 страницFault Tree Analysisankitsaxena123Оценок пока нет
- Quantitative Risk Analysis in The Chemical Process IndustryДокумент14 страницQuantitative Risk Analysis in The Chemical Process IndustryRonyОценок пока нет
- SHM - Practical 12 - Risk Assessment MethodsДокумент8 страницSHM - Practical 12 - Risk Assessment MethodsBhaliya AadityaОценок пока нет
- Fault Tree AnalysisДокумент7 страницFault Tree AnalysisthawdarОценок пока нет
- Risk-Based Inspection and Maintenance (RBIM) (Khan-Canada-2004)Документ14 страницRisk-Based Inspection and Maintenance (RBIM) (Khan-Canada-2004)juan diazОценок пока нет
- Root Cause Analysis: Ruksana Hamid, Medical Officer and Anesthesiologist, JK HealthДокумент7 страницRoot Cause Analysis: Ruksana Hamid, Medical Officer and Anesthesiologist, JK HealthAnar HajiyevОценок пока нет
- Comparison of Some Selected Methods For Accident Investigation PDFДокумент9 страницComparison of Some Selected Methods For Accident Investigation PDFSyifa AndalusiaОценок пока нет
- 1 s2.0 S0951832021003410 MainДокумент12 страниц1 s2.0 S0951832021003410 MainmkОценок пока нет
- Article Publié 10-1108 - IJQRM-03-2019-0078 PDFДокумент11 страницArticle Publié 10-1108 - IJQRM-03-2019-0078 PDFRachid SmailОценок пока нет
- Risk Analysis of Nuclear PowerДокумент11 страницRisk Analysis of Nuclear PowerAli KhalilОценок пока нет
- BSCATpaperassubmitteddec 82014Документ15 страницBSCATpaperassubmitteddec 82014Moroko69Оценок пока нет
- Five Fatal Flaws in API 581Документ12 страницFive Fatal Flaws in API 581Geert Henk WijnantsОценок пока нет
- Marx 2020Документ9 страницMarx 2020Gustavo AgudeloОценок пока нет
- Lecture 07 Risk AnalysisДокумент18 страницLecture 07 Risk Analysisrowan mamdouhОценок пока нет
- An Inherent Safety-Based Incident Investigation Methodology: Attiq Goraya, Paul R. Amyotte, and Faisal I. KhanДокумент9 страницAn Inherent Safety-Based Incident Investigation Methodology: Attiq Goraya, Paul R. Amyotte, and Faisal I. KhanValmir Pereira ZutinОценок пока нет
- Form A: Control Change Cause Analysis ManualДокумент20 страницForm A: Control Change Cause Analysis Manualmuratandac3357Оценок пока нет
- G 63 Quality Risk Management (QRM) Application For Critical Instrument CalibrationДокумент7 страницG 63 Quality Risk Management (QRM) Application For Critical Instrument CalibrationDoan Chi Thien100% (1)
- Safety Engineering: Felipe A. Arnejo Ii Sheila Marie C. Cagadas Jamelee S. Marzonia John Henry V. MoratallaДокумент11 страницSafety Engineering: Felipe A. Arnejo Ii Sheila Marie C. Cagadas Jamelee S. Marzonia John Henry V. MoratallaSheila Marie CagadasОценок пока нет
- Semi-Quantitative Fault Tree Analysis For Process Plant Safety Using Frequency and Probability RangesДокумент7 страницSemi-Quantitative Fault Tree Analysis For Process Plant Safety Using Frequency and Probability RangesRonak MotaОценок пока нет
- Engineering Failure Analysis: Ricardo Manuel Arias Velásquez, Jennifer Vanessa Mejía Lara, Andrés Melgar TДокумент25 страницEngineering Failure Analysis: Ricardo Manuel Arias Velásquez, Jennifer Vanessa Mejía Lara, Andrés Melgar TI Wayan ArimbawaОценок пока нет
- Using System Dynamics For Safety and Risk ManagemeДокумент11 страницUsing System Dynamics For Safety and Risk Manageme18rosa18Оценок пока нет
- Is.15656.2006 - Hazard Identification and Risk AssessmentДокумент31 страницаIs.15656.2006 - Hazard Identification and Risk Assessmentjitesh26100% (3)
- Iaea 2001 - Risk Informed Decision MakingДокумент37 страницIaea 2001 - Risk Informed Decision MakingOtso CronvallОценок пока нет
- NMISHRAG AppendicesДокумент48 страницNMISHRAG Appendicesapi-3733731Оценок пока нет
- Daftar Pustaka 2 (CCF)Документ36 страницDaftar Pustaka 2 (CCF)VikonuralfanОценок пока нет
- LPG Terminal SafetyДокумент4 страницыLPG Terminal SafetyIsioma1Оценок пока нет
- System Theory Based Hazard Analysis For Construction Site SafetyДокумент12 страницSystem Theory Based Hazard Analysis For Construction Site SafetymusniraОценок пока нет
- 1.1 BackgroundДокумент2 страницы1.1 BackgroundJonathan Cardenas100% (1)
- Domain 2 Management SystemДокумент125 страницDomain 2 Management SystemZohaib TahirОценок пока нет
- Near Miss Incidents in Chemical IndustryДокумент15 страницNear Miss Incidents in Chemical Industrychujiyo100% (1)
- Risk Analysis Methodology Applied To Industrial Machine DevelopmentДокумент8 страницRisk Analysis Methodology Applied To Industrial Machine DevelopmentHeliliano GuedesОценок пока нет
- Iec 61508Документ14 страницIec 61508Pandhu DewantoОценок пока нет
- Unit 4 HvpeДокумент12 страницUnit 4 HvpeRamОценок пока нет
- A Statistical Pattern Recognition Paradigm For Vibration-Based Structural Health MonitoringДокумент10 страницA Statistical Pattern Recognition Paradigm For Vibration-Based Structural Health Monitoringjun005Оценок пока нет
- Risk Assessment For Civil Engineering Facilities: Critical Overview and DiscussionДокумент12 страницRisk Assessment For Civil Engineering Facilities: Critical Overview and Discussionterror_ro533Оценок пока нет
- Probabilistic Radiological Risk Assessments For Radiation Facilities With Vague InformationДокумент11 страницProbabilistic Radiological Risk Assessments For Radiation Facilities With Vague InformationAyuОценок пока нет
- A Root Cause Analysis Method For Industrial Plant - Reliability Improvement and Engineering Design FeedbackДокумент6 страницA Root Cause Analysis Method For Industrial Plant - Reliability Improvement and Engineering Design FeedbackXiang LiuОценок пока нет
- Risk Assessment of Fishing Vessels: Ercan K OSE, A. Cemal D INC Er, H. Fehmi Durukano GLUДокумент11 страницRisk Assessment of Fishing Vessels: Ercan K OSE, A. Cemal D INC Er, H. Fehmi Durukano GLUmilad66tehОценок пока нет
- An Application of The Functional Resonance Analysis Method (FRAM) To Risk Assessment of Organisational CHДокумент87 страницAn Application of The Functional Resonance Analysis Method (FRAM) To Risk Assessment of Organisational CHvivianaОценок пока нет
- Of Chemical Reaction Systems: The State of The PracticeДокумент6 страницOf Chemical Reaction Systems: The State of The PracticeNambi PurushothОценок пока нет
- Comparison of Techniques For Accident Scenario Analysis in Hazardous SystemsДокумент9 страницComparison of Techniques For Accident Scenario Analysis in Hazardous SystemsSung Woo ShinОценок пока нет
- Sauf SIL Paper 4-99 (Public)Документ13 страницSauf SIL Paper 4-99 (Public)Ahmad AzabОценок пока нет
- 1 s2.0 S0925753522002570 MainДокумент14 страниц1 s2.0 S0925753522002570 MainneckitoОценок пока нет
- 1 s2.0 S2590123023005753 MainДокумент15 страниц1 s2.0 S2590123023005753 MainvdhivyaprabaОценок пока нет
- 02 - HAZID Techniques - Applications and LimitationsДокумент12 страниц02 - HAZID Techniques - Applications and Limitationsarman_morala100% (1)
- PL RA CH 4-143-164Документ22 страницыPL RA CH 4-143-164MAT-LIONОценок пока нет
- Reliability and Probabilistic Safety Assessment in Multi-Unit Nuclear Power PlantsОт EverandReliability and Probabilistic Safety Assessment in Multi-Unit Nuclear Power PlantsРейтинг: 5 из 5 звезд5/5 (1)
- Reliability, Maintainability and Risk: Practical Methods for EngineersОт EverandReliability, Maintainability and Risk: Practical Methods for EngineersРейтинг: 4.5 из 5 звезд4.5/5 (3)
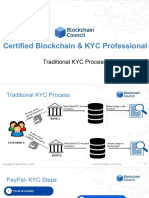
- Traditional KYC Process PDFДокумент5 страницTraditional KYC Process PDFvivxtractОценок пока нет
- Vadi 3Документ1 страницаVadi 3vivxtractОценок пока нет
- Public and Private KeyДокумент5 страницPublic and Private KeyvivxtractОценок пока нет
- Vadi 1Документ1 страницаVadi 1vivxtractОценок пока нет
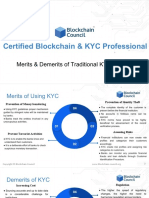
- Merits - Demerits of Traditional KYC Process PDFДокумент4 страницыMerits - Demerits of Traditional KYC Process PDFvivxtractОценок пока нет
- Vadi 2Документ1 страницаVadi 2vivxtractОценок пока нет
- 1 - Exam OverviewДокумент1 страница1 - Exam OverviewvivxtractОценок пока нет
- Amazon NG Photo Ark Book Invoice PDFДокумент1 страницаAmazon NG Photo Ark Book Invoice PDFvivxtractОценок пока нет
- What Is KYC - PDFДокумент6 страницWhat Is KYC - PDFvivxtractОценок пока нет
- Wstss Video InstructionsWSTSS Video InstructionsДокумент5 страницWstss Video InstructionsWSTSS Video InstructionsRobert PladetОценок пока нет
- A4 Brochure-Updated-24jan2018 PDFДокумент4 страницыA4 Brochure-Updated-24jan2018 PDFvivxtractОценок пока нет
- WelcomeДокумент13 страницWelcomeUdai ValluruОценок пока нет
- Introduction To CERTIFIED BLOCKCHAIN - KYC PROFESSIONAL PDFДокумент14 страницIntroduction To CERTIFIED BLOCKCHAIN - KYC PROFESSIONAL PDFvivxtractОценок пока нет
- CAMS Practice ExamДокумент37 страницCAMS Practice Examvivxtract100% (1)
- Military PFIДокумент81 страницаMilitary PFIvivxtractОценок пока нет
- 0 - Welcome LetterДокумент1 страница0 - Welcome LettervivxtractОценок пока нет
- Six Sigma Society: Exam Topics by BeltДокумент2 страницыSix Sigma Society: Exam Topics by BeltvivxtractОценок пока нет
- FATF Recommendations 2012 PDFДокумент134 страницыFATF Recommendations 2012 PDFFxTraderBrazilОценок пока нет
- 35 Imf Aml-CftДокумент2 страницы35 Imf Aml-CftvivxtractОценок пока нет
- 5 - Job TipsДокумент2 страницы5 - Job TipsvivxtractОценок пока нет
- ATT00001Документ1 страницаATT00001vivxtractОценок пока нет
- Impt TopicsДокумент1 страницаImpt TopicsvivxtractОценок пока нет
- Problem Structuring: The Process of Soda ModellingДокумент4 страницыProblem Structuring: The Process of Soda ModellingvivxtractОценок пока нет
- My YouTube PlaylistДокумент1 страницаMy YouTube PlaylistvivxtractОценок пока нет
- 165451819Документ7 страниц165451819vivxtractОценок пока нет
- Sights and Attractions Near London Eye - LondonTownДокумент4 страницыSights and Attractions Near London Eye - LondonTownvivxtractОценок пока нет
- ConclusionДокумент1 страницаConclusionvivxtractОценок пока нет
- Efficiency Hypothesis of The Stock Exchange Project Presented by MR CAMARA MOHAMED BINTOUДокумент113 страницEfficiency Hypothesis of The Stock Exchange Project Presented by MR CAMARA MOHAMED BINTOUCamara Mohamed Bintou100% (1)
- Man-Made Disaster - Nuclear DisasterДокумент23 страницыMan-Made Disaster - Nuclear Disasterpratham sainiОценок пока нет
- 26053027Документ350 страниц26053027guerrezОценок пока нет
- Presentation 6 Fukushima Nuclear Power Plant Accident Imperial College London Sae OchiДокумент26 страницPresentation 6 Fukushima Nuclear Power Plant Accident Imperial College London Sae OchiKlea RoseniОценок пока нет
- EAF Energy ModelДокумент10 страницEAF Energy Modelcimav100% (2)
- Francis Tenazas Nuclear Power PointДокумент20 страницFrancis Tenazas Nuclear Power PointStephanie TenazasОценок пока нет
- Accidents, Leaks, Failures and Other Incidents in The Nuclear Industrial and MilitaryДокумент154 страницыAccidents, Leaks, Failures and Other Incidents in The Nuclear Industrial and MilitaryTroy LivingstonОценок пока нет
- Fukushima Meltdown & Modern RadiationДокумент216 страницFukushima Meltdown & Modern RadiationJohn OliphantОценок пока нет
- Physics: Department of EducationДокумент16 страницPhysics: Department of EducationIsrael PopeОценок пока нет
- 2011 05 15 Epearl - Lord HimalayaДокумент5 страниц2011 05 15 Epearl - Lord HimalayaAbraham DIKAОценок пока нет
- Standard Review Plan: NRO - SRP@NRC - GovДокумент44 страницыStandard Review Plan: NRO - SRP@NRC - GovSivakumar LОценок пока нет
- 1.A - EPR Design Description - v3 PDFДокумент185 страниц1.A - EPR Design Description - v3 PDFMudassarHashmiОценок пока нет
- AP1000 Nuclear Power Plant Overview Gianfranco Saiu, Monica Linda FrogheriДокумент21 страницаAP1000 Nuclear Power Plant Overview Gianfranco Saiu, Monica Linda FrogheriKonathala RajashekarОценок пока нет
- Koodankulam Nuclear Power PlantДокумент15 страницKoodankulam Nuclear Power PlantEdgardo SimpsonОценок пока нет
- Chapter 19Документ262 страницыChapter 19hidayat222222Оценок пока нет
- 9-11 An Analysis of The US Geological Survey Data - Ground Zero-The Nuclear Destruction of The WTC - William TahilДокумент19 страниц9-11 An Analysis of The US Geological Survey Data - Ground Zero-The Nuclear Destruction of The WTC - William Tahilsvinche4100% (1)
- Costa Hosh - SP Final DraftДокумент10 страницCosta Hosh - SP Final Draftapi-551407564Оценок пока нет
- Intercorp 3.0Документ51 страницаIntercorp 3.0Alif AnasОценок пока нет
- Report On Failure Modes in Reactor Pressure Vessel - IncompleteДокумент20 страницReport On Failure Modes in Reactor Pressure Vessel - IncompleteSai NathОценок пока нет
- Schelling What Purposes Can International Terrorism ServeДокумент15 страницSchelling What Purposes Can International Terrorism ServeJakob StimmlerОценок пока нет
- Hazarde IndustrialeДокумент21 страницаHazarde IndustrialeFecheta CiprianОценок пока нет
- Methodology Risk FireДокумент412 страницMethodology Risk FireingatvОценок пока нет
- Shadowrun Timeline Full Up To 2077Документ48 страницShadowrun Timeline Full Up To 2077Luis Fernando Telles DajelloОценок пока нет
- Lancer - Cheat SheetДокумент11 страницLancer - Cheat Sheettriple zeeОценок пока нет
- Essay Source Book1 PDFДокумент426 страницEssay Source Book1 PDFTraian MantarosieОценок пока нет
- IAEA SMR Booklet 2014 PDFДокумент150 страницIAEA SMR Booklet 2014 PDF302345Оценок пока нет
- 2022 Disaster Management Students Notes Lecture 1 2 and 3Документ98 страниц2022 Disaster Management Students Notes Lecture 1 2 and 3Edwin AkhwaleОценок пока нет
- 2012 - Status of SMR Design NENP NPTDS PDFДокумент90 страниц2012 - Status of SMR Design NENP NPTDS PDFskylancer-3441Оценок пока нет
- Science - 4 March 2016 PDFДокумент138 страницScience - 4 March 2016 PDFMarkCaniculaОценок пока нет
- Chemtrails & Winter Illness-In ProcessДокумент9 страницChemtrails & Winter Illness-In ProcessKlaudiko IlgabibichОценок пока нет