Вам также может понравиться
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- SD OverviewДокумент85 страницSD OverviewSamatha GantaОценок пока нет
- Roman Catholic Bishop of Jaro v. Dela PenaДокумент2 страницыRoman Catholic Bishop of Jaro v. Dela PenaBeltran KathОценок пока нет
- Classroom Management PaperДокумент7 страницClassroom Management PaperdessyutamiОценок пока нет
- Grenade FINAL (Esl Song Activities)Документ4 страницыGrenade FINAL (Esl Song Activities)Ti LeeОценок пока нет
- Course-Outline EL 102 GenderAndSocietyДокумент4 страницыCourse-Outline EL 102 GenderAndSocietyDaneilo Dela Cruz Jr.Оценок пока нет
- Cell Bio1Документ7 страницCell Bio1AnyaОценок пока нет
- Top Websites Ranking - Most Visited Websites in May 2023 - SimilarwebДокумент3 страницыTop Websites Ranking - Most Visited Websites in May 2023 - SimilarwebmullahОценок пока нет
- Let's Try This: Incident: Thoughts: Feelings: Behavior: Incident: Thoughts: Feelings: BehaviorДокумент2 страницыLet's Try This: Incident: Thoughts: Feelings: Behavior: Incident: Thoughts: Feelings: BehaviorJannet Viacruses LarcenaОценок пока нет
- Network Firewall SecurityДокумент133 страницыNetwork Firewall Securitysagar323Оценок пока нет
- Ais Activiy Chapter 5 PDFДокумент4 страницыAis Activiy Chapter 5 PDFAB CloydОценок пока нет
- Invoice Ce 2019 12 IVДокумент8 страницInvoice Ce 2019 12 IVMoussa NdourОценок пока нет
- Rath'S Lectures: Longevity Related Notes On Vimsottari DasaДокумент5 страницRath'S Lectures: Longevity Related Notes On Vimsottari DasasudhinnnОценок пока нет
- Academic Calendar 2014 15Документ6 страницAcademic Calendar 2014 15D Geetha DuraiОценок пока нет
- Reseller Handbook 2019 v1Документ16 страницReseller Handbook 2019 v1Jennyfer SantosОценок пока нет
- Crim Pro Exam Sheet at A Glance.Документ5 страницCrim Pro Exam Sheet at A Glance.Heather Kinsaul Foster80% (5)
- Sections 3 7Документ20 страницSections 3 7ninalgamaryroseОценок пока нет
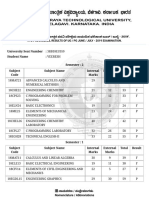
- VTU Result PDFДокумент2 страницыVTU Result PDFVaibhavОценок пока нет
- Chapter 2 Organizational Behavior - Robbins, JudgeДокумент3 страницыChapter 2 Organizational Behavior - Robbins, JudgeRes Gosan100% (2)
- GEHealthcare Brochure - Discovery CT590 RT PDFДокумент12 страницGEHealthcare Brochure - Discovery CT590 RT PDFAnonymous ArdclHUOОценок пока нет
- Percussion Digital TWДокумент26 страницPercussion Digital TWAlberto GallardoОценок пока нет
- Linear Arrangement 3rdДокумент30 страницLinear Arrangement 3rdSonu BishtОценок пока нет
- ART 6 LEARNING PACKET Week2-3Документ10 страницART 6 LEARNING PACKET Week2-3Eljohn CabantacОценок пока нет
- RECAP Lecture 7: FA of EVEN EVEN, FA Corresponding To Finite Languages (Using Both Methods), Transition GraphsДокумент23 страницыRECAP Lecture 7: FA of EVEN EVEN, FA Corresponding To Finite Languages (Using Both Methods), Transition GraphsMuhammad EahteshamОценок пока нет
- Superscope, Inc. v. Brookline Corp., Etc., Robert E. Lockwood, 715 F.2d 701, 1st Cir. (1983)Документ3 страницыSuperscope, Inc. v. Brookline Corp., Etc., Robert E. Lockwood, 715 F.2d 701, 1st Cir. (1983)Scribd Government DocsОценок пока нет
- Journal of Cleaner Production: Kamalakanta Muduli, Kannan Govindan, Akhilesh Barve, Yong GengДокумент10 страницJournal of Cleaner Production: Kamalakanta Muduli, Kannan Govindan, Akhilesh Barve, Yong GengAnass CHERRAFIОценок пока нет
- NB-CPD IR 4r1 - Guidance For SGs On Their Role and Working MethodsДокумент19 страницNB-CPD IR 4r1 - Guidance For SGs On Their Role and Working MethodsmingulОценок пока нет
- Dermatome, Myotome, SclerotomeДокумент4 страницыDermatome, Myotome, SclerotomeElka Rifqah100% (3)
- Eco - Module 1 - Unit 3Документ8 страницEco - Module 1 - Unit 3Kartik PuranikОценок пока нет
- Anecdotal Records For Piano Methods and Piano BooksДокумент5 страницAnecdotal Records For Piano Methods and Piano BooksCes Disini-PitogoОценок пока нет
- Operations Management and Operations PerformanceДокумент59 страницOperations Management and Operations PerformancePauline LagtoОценок пока нет