Вам также может понравиться
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Quickbooks Online CertificatДокумент137 страницQuickbooks Online CertificatRandy Fernandez100% (6)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Phone Bill Jan 2022Документ6 страницPhone Bill Jan 2022Maxime VogneОценок пока нет
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Financial Crimes Reporting Form: Grand Junction Police DepartmentДокумент6 страницFinancial Crimes Reporting Form: Grand Junction Police Departmentheather valenzuelaОценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Mercantile Law Bar Exam Q&AДокумент26 страницMercantile Law Bar Exam Q&AVerdeth Marie Wagan100% (1)
- Activity Balancing Your Checking AccountДокумент4 страницыActivity Balancing Your Checking AccountMellanie Garcia100% (1)
- The Negotiable Instruments ActДокумент20 страницThe Negotiable Instruments Actpooja guptaОценок пока нет
- T-Codes of Sap REMДокумент14 страницT-Codes of Sap REMskanth248Оценок пока нет
- Cash Management ProjectДокумент74 страницыCash Management ProjectDinesh Kumar Karur77% (78)
- Make My TripДокумент94 страницыMake My TripRohit YadavОценок пока нет
- Application For Convocation 56709 NASHI YUVRAJ RAJSHEKHARДокумент2 страницыApplication For Convocation 56709 NASHI YUVRAJ RAJSHEKHARRajОценок пока нет
- Metropolitan Bank & Trust Co. v. B.A. FinanceДокумент2 страницыMetropolitan Bank & Trust Co. v. B.A. FinanceNiajhan PalattaoОценок пока нет
- VCB-ib@nking User Guide PDFДокумент34 страницыVCB-ib@nking User Guide PDFThông Hà ThúcОценок пока нет
- STP Analysis For ICICI BankДокумент27 страницSTP Analysis For ICICI BankRohit Jain100% (1)
- Banking Vocabulary and ExpressionsДокумент2 страницыBanking Vocabulary and Expressionsrussell_diamondОценок пока нет
- Session 1 - Introduction To BankingДокумент65 страницSession 1 - Introduction To BankingMohamed AhmedОценок пока нет
- Aliner KitsДокумент5 страницAliner KitsthriftytravelОценок пока нет
- Bank Reconciliation ActivitiesДокумент1 страницаBank Reconciliation Activitiesmaligaya evelynОценок пока нет
- Unit 5 DIGITALMARKETING AND E COMMERCEДокумент16 страницUnit 5 DIGITALMARKETING AND E COMMERCESUFIYAN KHANОценок пока нет
- Thu HienДокумент5 страницThu Hienanon_26346252Оценок пока нет
- Westmont Bank (Formerly Associated Banking Corp.) vs. Eugene Ong GR No. 132560, January 30, 2002 FactsДокумент54 страницыWestmont Bank (Formerly Associated Banking Corp.) vs. Eugene Ong GR No. 132560, January 30, 2002 FactsKrystalynne AguilarОценок пока нет
- Amverton Heritage Resort, Ayer KerohДокумент4 страницыAmverton Heritage Resort, Ayer KerohJohn IlyasОценок пока нет
- Modified Vendor Registration Form PDFДокумент3 страницыModified Vendor Registration Form PDFAnonymous cKGCdi100% (1)
- Final Askari Bank Report HamzaДокумент41 страницаFinal Askari Bank Report HamzaSO HaОценок пока нет
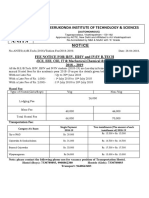
- Anil Neerukonda Institute of Technology & Sciences: Fee Notice For Ii/Iv, Iii/Iv and Iv/Iv B.Tech 2018 - 2019Документ3 страницыAnil Neerukonda Institute of Technology & Sciences: Fee Notice For Ii/Iv, Iii/Iv and Iv/Iv B.Tech 2018 - 2019p.narendraОценок пока нет
- CBQ Termsandconditions en 3102011Документ81 страницаCBQ Termsandconditions en 3102011ahmed50alasalОценок пока нет
- Client Ledger V 10Документ11 страницClient Ledger V 10Julieth TeembaОценок пока нет
- Instructions:: Assignmnet 2 - Chapter 7 (Petty Cash & Bank Reconciliation)Документ5 страницInstructions:: Assignmnet 2 - Chapter 7 (Petty Cash & Bank Reconciliation)Success LibraryОценок пока нет
- FlightДокумент2 страницыFlightMalai SelvanОценок пока нет
- Quick Reference For CRM NPC (Manual Order) : Phone Service Service As Wire Line, Service Type As LandlineДокумент6 страницQuick Reference For CRM NPC (Manual Order) : Phone Service Service As Wire Line, Service Type As LandlineGangadhar Reddy TavvaОценок пока нет
- Recent Trends and Development of Banking System in IndiaДокумент5 страницRecent Trends and Development of Banking System in Indiavishnu priya v 149Оценок пока нет