Вам также может понравиться
- Community Acquired Pneumonia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОт EverandCommunity Acquired Pneumonia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОценок пока нет
- Pamantasan NG Cabuyao College of Health Allied Sciences College of NursingДокумент43 страницыPamantasan NG Cabuyao College of Health Allied Sciences College of NursingSofea MustaffaОценок пока нет
- Case Study 2.odtДокумент10 страницCase Study 2.odtAlejandro Daniel Landa Morales100% (1)
- Assessment Diagnosis Goals and Objectives Planning Intervention Rationale EvaluationДокумент3 страницыAssessment Diagnosis Goals and Objectives Planning Intervention Rationale EvaluationCrissa AngelОценок пока нет
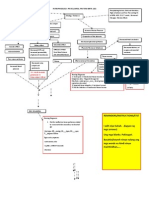
- Pathophysiology (Client Base) :: Predisposing Factors: Precipitating FactorsДокумент1 страницаPathophysiology (Client Base) :: Predisposing Factors: Precipitating Factorsleslie_macasaetОценок пока нет
- N. Bacalso Ave., Cebu City Philippines: Page 1 of 32Документ32 страницыN. Bacalso Ave., Cebu City Philippines: Page 1 of 32Joule PeirreОценок пока нет
- Concept Map On Acute PainДокумент1 страницаConcept Map On Acute PainKatherine Conlu Bengan0% (1)
- AAДокумент20 страницAAAiyaz AliОценок пока нет
- Placenta Previa PathoДокумент2 страницыPlacenta Previa Pathoshakira0% (1)
- Hydatidiform Mole: PGI Sia, Kevin PGI Tan, SheilaДокумент80 страницHydatidiform Mole: PGI Sia, Kevin PGI Tan, SheilaSheila Mary TanОценок пока нет
- Pa Tho Physiology of RaДокумент7 страницPa Tho Physiology of Ralisalmar2008Оценок пока нет
- CASE STUDY PheumoniaДокумент5 страницCASE STUDY PheumoniaEdelweiss Marie CayetanoОценок пока нет
- JRMMC - Patho of Ruptured AppendicitisДокумент3 страницыJRMMC - Patho of Ruptured Appendicitis9632141475963Оценок пока нет
- Pathophysiology: Cholecystitis Non Modifiable Factors Modifiable FactorsДокумент4 страницыPathophysiology: Cholecystitis Non Modifiable Factors Modifiable FactorsLovely DaroleОценок пока нет
- Physical Examination and Review of Systems: Peri-Orbital Hematoma Sub-Conjunctiva Hemorrhage On Left EyeДокумент3 страницыPhysical Examination and Review of Systems: Peri-Orbital Hematoma Sub-Conjunctiva Hemorrhage On Left EyeBianx Flores DosdosОценок пока нет
- Buergers Power PointДокумент16 страницBuergers Power PointYan VencerОценок пока нет
- Influenza PATHOPHYSIOLOGYДокумент3 страницыInfluenza PATHOPHYSIOLOGYElle RosalesОценок пока нет
- CPD Concept MapДокумент1 страницаCPD Concept MapShandle Dynne BaenaОценок пока нет
- AGE With Pa Tho PhysiologyДокумент3 страницыAGE With Pa Tho PhysiologyChichi Licuben OresacamОценок пока нет
- Pathophysiology of Ruptured Ectopic PregnancyДокумент3 страницыPathophysiology of Ruptured Ectopic Pregnancybowki namoОценок пока нет
- EndometriosisДокумент6 страницEndometriosissalamredОценок пока нет
- Unit 1 5AДокумент7 страницUnit 1 5AArvin O-CaféОценок пока нет
- Name of Drug Mechanism of Action Indication Contraindication Side Effects Adverse Effects Nursing Consideration IndicationДокумент2 страницыName of Drug Mechanism of Action Indication Contraindication Side Effects Adverse Effects Nursing Consideration IndicationBrian BaggayanОценок пока нет
- Chronic PyelonephritisДокумент5 страницChronic PyelonephritisIsak ShatikaОценок пока нет
- Pathophysiology of PihДокумент3 страницыPathophysiology of PihMargueretti Delos ReyesОценок пока нет
- Pathophysiology Precipitsting Factors: Predisposing FactorsДокумент2 страницыPathophysiology Precipitsting Factors: Predisposing FactorsGeofrey MaglalangОценок пока нет
- Thyroid Papillary Carcinoma CaseДокумент6 страницThyroid Papillary Carcinoma CaseRandy F BabaoОценок пока нет
- Preeclampsia Pathophysiology and ManagementДокумент7 страницPreeclampsia Pathophysiology and ManagementAuliaОценок пока нет
- Adenomyosis PathophysiologyДокумент1 страницаAdenomyosis PathophysiologyZerfa NishreenОценок пока нет
- Cervical IncompetenceДокумент30 страницCervical IncompetenceSignor ArasОценок пока нет
- Modifiedpatho ToyodaДокумент4 страницыModifiedpatho ToyodaCaneEscabarteОценок пока нет
- NCPДокумент10 страницNCPRobin HaliliОценок пока нет
- Patho of CA & Breast CaДокумент3 страницыPatho of CA & Breast CaAngeline EspinasОценок пока нет
- GastroschisisДокумент19 страницGastroschisiskunaidongОценок пока нет
- Acute TonsillopharyngitisДокумент17 страницAcute TonsillopharyngitisRachel Haide NaravalОценок пока нет
- Case Study CSДокумент21 страницаCase Study CSThessa Lonica GarciaОценок пока нет
- Case Scenario Dengue FeverДокумент2 страницыCase Scenario Dengue FeverJaslir MendozaОценок пока нет
- Epidemiology, Pathogenesis, and Pathology of NeuroblastomaДокумент21 страницаEpidemiology, Pathogenesis, and Pathology of NeuroblastomaHandre PutraОценок пока нет
- Casestudy Makato 2nd Pre EclampsiaДокумент7 страницCasestudy Makato 2nd Pre EclampsiaRainier IbarretaОценок пока нет
- Schistosomiasis (From Anatomy To Pathophysiology)Документ10 страницSchistosomiasis (From Anatomy To Pathophysiology)Tiger Knee100% (1)
- FNCP FinaaaalДокумент5 страницFNCP FinaaaalSoniaMarieBalanay0% (1)
- Pa Tho Physiology of OsteoporosisДокумент2 страницыPa Tho Physiology of Osteoporosisjcam_o9Оценок пока нет
- Nursing Care Plan: Subjective: Nabalaka Ko Short Term: Independent: Goal Met Short TermДокумент3 страницыNursing Care Plan: Subjective: Nabalaka Ko Short Term: Independent: Goal Met Short Termgeng gengОценок пока нет
- Pathophysiology AppendicitisДокумент3 страницыPathophysiology AppendicitisIra Krystel ReyesОценок пока нет
- Discharge PlanДокумент4 страницыDischarge PlanPaul Loujin LeeОценок пока нет
- Pathophysiology of Transitional Cell CarcinomaДокумент10 страницPathophysiology of Transitional Cell CarcinomaJheanAlphonsineT.MeansОценок пока нет
- Upper Respiratory Tract InfectionДокумент12 страницUpper Respiratory Tract InfectionErmie BalingitОценок пока нет
- Case Pres A1-RhdДокумент11 страницCase Pres A1-RhdCharm TanyaОценок пока нет
- Gestational Thropoblastic DiseaseДокумент56 страницGestational Thropoblastic DiseaseGringo Barroga0% (1)
- Case Study FormatДокумент5 страницCase Study FormatEden OlasabОценок пока нет
- H MoleДокумент2 страницыH MoleJoanna Marie Datahan EstomoОценок пока нет
- Intussusception: PathophysiologyДокумент8 страницIntussusception: PathophysiologyNaufal AndaluОценок пока нет
- Acute Cholecystitis SeminarДокумент42 страницыAcute Cholecystitis SeminarNatnaelОценок пока нет
- Pathophysiology (Risk Factors & Symptoms)Документ20 страницPathophysiology (Risk Factors & Symptoms)Ann Michelle TarrobagoОценок пока нет
- Placino HIRSCHPRUNG DX PDFДокумент15 страницPlacino HIRSCHPRUNG DX PDFSiena PlacinoОценок пока нет
- Diabetes PathoДокумент2 страницыDiabetes Pathodrewcel100% (1)
- Hirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОт EverandHirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОценок пока нет
- Acute EpiglottisДокумент20 страницAcute EpiglottissuciОценок пока нет
- Bacterial Causes of URIДокумент28 страницBacterial Causes of URIOmar MohammedОценок пока нет
- The Biography of Hazrat Khwaja Usman HarooniДокумент6 страницThe Biography of Hazrat Khwaja Usman HarooniMohammed Abdul Hafeez, B.Com., Hyderabad, IndiaОценок пока нет
- Objectives:: Course Name: Islamic Studies Course Structure: Lectures: 3, Labs: 0 Credit Hours: 3 Prerequisites: NoneДокумент3 страницыObjectives:: Course Name: Islamic Studies Course Structure: Lectures: 3, Labs: 0 Credit Hours: 3 Prerequisites: Nonescam xdОценок пока нет
- R. v. Ituluk, 2018 NUCJ 21Документ7 страницR. v. Ituluk, 2018 NUCJ 21NunatsiaqNewsОценок пока нет
- Muslim Women's Quest For Equality Between Islamic Law and Feminism - Ziba Mir Hosseini - ChicagoДокумент18 страницMuslim Women's Quest For Equality Between Islamic Law and Feminism - Ziba Mir Hosseini - Chicagooohdeem oohdeemОценок пока нет
- 1.2 Nasser's Consolidation of Power: ScrollДокумент4 страницы1.2 Nasser's Consolidation of Power: ScrollI LytssОценок пока нет
- 041 - SPH - Raj - X - 20 - MR Variation Order Line Detector & Mcfa Integration (09102020)Документ3 страницы041 - SPH - Raj - X - 20 - MR Variation Order Line Detector & Mcfa Integration (09102020)Andy SanjayaОценок пока нет
- Index (2014)Документ3 905 страницIndex (2014)NocoJoeОценок пока нет
- Generalized Anxiety DisorderДокумент73 страницыGeneralized Anxiety DisorderBincy KurianОценок пока нет
- ANG TIBAY v. CIRДокумент2 страницыANG TIBAY v. CIRMa Gabriellen Quijada-Tabuñag80% (5)
- Text Di Bawah Ini Digunakan Untuk Menjawab Nomor 1 Dan 2.: Rahmat and Wati JumintenДокумент3 страницыText Di Bawah Ini Digunakan Untuk Menjawab Nomor 1 Dan 2.: Rahmat and Wati JumintenKiddy Care TegalОценок пока нет
- Guardianship Spec ProДокумент2 страницыGuardianship Spec ProCedrick Contado Susi BocoОценок пока нет
- State of Israel: Full Name of The CountryДокумент7 страницState of Israel: Full Name of The CountryËs Gue Rra YshëënОценок пока нет
- 6.1 Classification Board and Disciplinary BoardДокумент4 страницы6.1 Classification Board and Disciplinary BoardKaneki KenОценок пока нет
- ChagosДокумент10 страницChagosFabrice FlochОценок пока нет
- Remedies OutlineДокумент95 страницRemedies Outlinebbastoky_690257214100% (2)
- Principles of Forensic ScienceДокумент6 страницPrinciples of Forensic SciencepranjalОценок пока нет
- CHAPTER 1 THE EARLY HISTORY OF MALAYSIA - September 2018Документ119 страницCHAPTER 1 THE EARLY HISTORY OF MALAYSIA - September 2018MD HOSSAINОценок пока нет
- History of Arnis EssayДокумент2 страницыHistory of Arnis EssayNatss VillanuevaОценок пока нет
- Notes From Discover Canada - Preparation For The Citizenship Test - Canada Immigration ForumДокумент2 страницыNotes From Discover Canada - Preparation For The Citizenship Test - Canada Immigration ForumGowtham SubramanianОценок пока нет
- If I Were You NotesДокумент5 страницIf I Were You NotesHima BinduОценок пока нет
- GR. No. L-38429 June 30, 1988Документ2 страницыGR. No. L-38429 June 30, 1988nyc enguitoОценок пока нет
- Webster MTDДокумент18 страницWebster MTDStopGovt WasteОценок пока нет
- Labor Standards CasesДокумент72 страницыLabor Standards CasesCarmel LouiseОценок пока нет
- tkr304p 2019feb PDFДокумент1 страницаtkr304p 2019feb PDFBenmar Coronado100% (1)
- Jamnalal Bajaj Institute of Management: Telgi ScamДокумент14 страницJamnalal Bajaj Institute of Management: Telgi ScamAnkita DesaiОценок пока нет
- Bpop Plan - DanahaoДокумент3 страницыBpop Plan - DanahaoJessica CindyОценок пока нет
- A Strategic Plan For Empowering Pakistan's Civil Society To Counter Violent Extremism (WORDE, 2015)Документ20 страницA Strategic Plan For Empowering Pakistan's Civil Society To Counter Violent Extremism (WORDE, 2015)Ghulam MustafaОценок пока нет
- Letter To President Biden From New York Assemblymember Bichotte With Respect To HaitiДокумент3 страницыLetter To President Biden From New York Assemblymember Bichotte With Respect To HaitiSabrina RezzyОценок пока нет
- People Vs DacilloДокумент6 страницPeople Vs Dacillogeorgina616Оценок пока нет
- Music Guide SupernaturalДокумент7 страницMusic Guide SupernaturalEl WahyudiОценок пока нет