Вам также может понравиться
- Myofascial ReleaseДокумент8 страницMyofascial Releaseprokin_martinezОценок пока нет
- Orthopaedic Management in Cerebral Palsy, 2nd EditionОт EverandOrthopaedic Management in Cerebral Palsy, 2nd EditionHelen Meeks HorstmannРейтинг: 3 из 5 звезд3/5 (2)
- CP PDFДокумент7 страницCP PDFannaОценок пока нет
- Sense Organ:vestibular OrganДокумент55 страницSense Organ:vestibular OrganivanОценок пока нет
- Clinical Neurodynamics and Sports Medicine: Origins and DevelopmentДокумент8 страницClinical Neurodynamics and Sports Medicine: Origins and DevelopmentWahid NasrudinОценок пока нет
- Therapybook Interferencial TherapyДокумент34 страницыTherapybook Interferencial TherapyBrian RaymondОценок пока нет
- Pathophysiology of Spastic Paresis IДокумент17 страницPathophysiology of Spastic Paresis Ivarahamihir100% (2)
- Physical Therapy Clinical ManagementДокумент24 страницыPhysical Therapy Clinical ManagementClaudia MicuОценок пока нет
- Understanding The Stretch ReflexДокумент2 страницыUnderstanding The Stretch ReflexJingyan ZhangОценок пока нет
- Poster PresentationДокумент1 страницаPoster PresentationAayat KhanОценок пока нет
- Neurostimulation For Stroke RehabilitationДокумент11 страницNeurostimulation For Stroke Rehabilitationisos.mporei.vevaios.Оценок пока нет
- Advances in Spinal Stabilization PDFДокумент333 страницыAdvances in Spinal Stabilization PDFMateo CortesОценок пока нет
- Pain Science in PracticeДокумент4 страницыPain Science in PracticeIan PeroniОценок пока нет
- AP41 MДокумент3 страницыAP41 Monix2000Оценок пока нет
- Normal Human LocomotionДокумент16 страницNormal Human LocomotionWendy NgОценок пока нет
- Mirror Therapy PDFДокумент26 страницMirror Therapy PDFrusu_alexandra_4Оценок пока нет
- Physiotherapy's Role in Managing Spasticity for Children with Cerebral PalsyДокумент3 страницыPhysiotherapy's Role in Managing Spasticity for Children with Cerebral PalsyKhusnah KhauliyaОценок пока нет
- Bogduk 2009Документ3 страницыBogduk 2009Borys100% (1)
- Form 4 Science Chapter 2.4 & 2.5 Muscle, Tendon, Ligament and BrainДокумент32 страницыForm 4 Science Chapter 2.4 & 2.5 Muscle, Tendon, Ligament and BraincmeeflyОценок пока нет
- Physio Shacklock 95Документ8 страницPhysio Shacklock 95Raihan HabibОценок пока нет
- Amputee Activity Score PDFДокумент5 страницAmputee Activity Score PDFLydia MartínОценок пока нет
- Makalah Bobath Approach For Adult With Neurological ConditionsДокумент54 страницыMakalah Bobath Approach For Adult With Neurological ConditionsArin SupriyadiОценок пока нет
- Proprioceptive Neuromuscular Facilitation (PNF) Stretching Techniques Hold-Relax HR ALLДокумент8 страницProprioceptive Neuromuscular Facilitation (PNF) Stretching Techniques Hold-Relax HR ALLKiné Therapeut-manuelle Masseur GabiОценок пока нет
- Autonomic Nervous System: DR S S Ranasinghe CNTH - RagamaДокумент63 страницыAutonomic Nervous System: DR S S Ranasinghe CNTH - RagamawellawalalasithОценок пока нет
- 2012 Scapular-Focused Treatment in Patients With ShoulderДокумент13 страниц2012 Scapular-Focused Treatment in Patients With ShoulderIsrael Matías Chandia Ramírez100% (1)
- Proprioceptive Neuromuscular Facilitation: Vicky S. WardlawДокумент44 страницыProprioceptive Neuromuscular Facilitation: Vicky S. WardlawPraneetha Nouduri100% (1)
- Hemispatial Neglect LDHДокумент20 страницHemispatial Neglect LDHAldersleyОценок пока нет
- Rehabilitation of LeprosyДокумент72 страницыRehabilitation of LeprosyNur OctavianiОценок пока нет
- KNTU NeuroMuscularSys 2018 MuscleSpindle SYariДокумент15 страницKNTU NeuroMuscularSys 2018 MuscleSpindle SYarisantiago mejia100% (1)
- NKT FlowChart - PDF Version 1 PDFДокумент2 страницыNKT FlowChart - PDF Version 1 PDFJay SarkОценок пока нет
- Vonpiekartz2020 PDFДокумент18 страницVonpiekartz2020 PDFKinjal SharmaОценок пока нет
- Hip Displacement in Cerebral PalsyДокумент9 страницHip Displacement in Cerebral PalsyJohannesSchoppmannОценок пока нет
- Eng Tecar-Crv-200 Rev1 LRДокумент36 страницEng Tecar-Crv-200 Rev1 LRThe LamОценок пока нет
- Kaltenborn Evjenth Concept of OMTДокумент34 страницыKaltenborn Evjenth Concept of OMTJaan100% (1)
- Tendon Neuroplastic TrainingДокумент9 страницTendon Neuroplastic TrainingLara VitorОценок пока нет
- Duque2021 Article OsteosarcopeniaAGeriatricGiantДокумент4 страницыDuque2021 Article OsteosarcopeniaAGeriatricGiantVERONICA BARRERAОценок пока нет
- Foot DropДокумент64 страницыFoot DropRam Chandra Reddy100% (1)
- The Helical Ventricular Myocardial Band of Torrent-GuaspДокумент5 страницThe Helical Ventricular Myocardial Band of Torrent-GuaspTeaKovacevicОценок пока нет
- Diagnostic Touch Its Principles and Application PDFДокумент9 страницDiagnostic Touch Its Principles and Application PDFJakobStierleОценок пока нет
- Jakarta School of Prosthetics & Orthotics: Upper Limb Prosthetics Course Work Manual 2010Документ84 страницыJakarta School of Prosthetics & Orthotics: Upper Limb Prosthetics Course Work Manual 2010Adinda Dinda100% (1)
- Motor Control PDFДокумент19 страницMotor Control PDFsurabhi_lodha8709Оценок пока нет
- Bobath For Musculoskeletal Problem Palembang Online 2020Документ128 страницBobath For Musculoskeletal Problem Palembang Online 2020fisioterapi rsph100% (1)
- Neural Control and Upper Limb RehabilitationДокумент6 страницNeural Control and Upper Limb RehabilitationDavid Camilo PinzonОценок пока нет
- Kinetic Control Cap1Документ17 страницKinetic Control Cap1Yennifer Serna MoncadaОценок пока нет
- Manual Muscle Testing of Infants, Toddlers, & Preschool ChildrenДокумент7 страницManual Muscle Testing of Infants, Toddlers, & Preschool Childrendeasy100% (1)
- Freedom To Move: Movement Therapy For Spinal Pain and Injuries - DanceДокумент5 страницFreedom To Move: Movement Therapy For Spinal Pain and Injuries - DancemofakiboОценок пока нет
- Corelation Muscle Strength and Balance 2016Документ5 страницCorelation Muscle Strength and Balance 2016Noribel Juarez MadridОценок пока нет
- Chapter 10 - Trigeminal NeuralgiaДокумент5 страницChapter 10 - Trigeminal NeuralgiaMuhammad IkbarОценок пока нет
- Pelvic Fractures - These Can Kill YouДокумент20 страницPelvic Fractures - These Can Kill YouSurgicalgownОценок пока нет
- ACBT and Autogenic Drainage PDFДокумент14 страницACBT and Autogenic Drainage PDFSwati GuptaОценок пока нет
- Chiropractic Subluxation Assessment - What The Research Tells Us - Edward F Owens, Jr.Документ6 страницChiropractic Subluxation Assessment - What The Research Tells Us - Edward F Owens, Jr.YuldashОценок пока нет
- The Bioenergetic Model in Osteopathic Diagnosis and Treatment: An FAAO Thesis, Part 1Документ9 страницThe Bioenergetic Model in Osteopathic Diagnosis and Treatment: An FAAO Thesis, Part 1nish0420100% (1)
- Physical Examination of The SpineДокумент33 страницыPhysical Examination of The SpineyudiОценок пока нет
- Spinal Segmental Sensitization As A Common OriginДокумент8 страницSpinal Segmental Sensitization As A Common OriginRossangel Huapaya RomeroОценок пока нет
- Sensorimotor Integration For FunctionalДокумент17 страницSensorimotor Integration For FunctionalFuncionalidad DiversaОценок пока нет
- Diaphragm Sparing Brachial Plexus Blocks A.12Документ7 страницDiaphragm Sparing Brachial Plexus Blocks A.12FIA SlotОценок пока нет
- Low Back Pain ICD-10 Code M54.5Документ1 страницаLow Back Pain ICD-10 Code M54.5fisioterapi 2019Оценок пока нет
- Godman - 1824 - Fascia of The Human BodyДокумент27 страницGodman - 1824 - Fascia of The Human BodyDustin LimaОценок пока нет
- An Appreciation of Sherrington's "The Integrative Action of The Nervous System"Документ8 страницAn Appreciation of Sherrington's "The Integrative Action of The Nervous System"saswepakОценок пока нет
- Functional Rehabilitation of Low Back Pain With Core StabilizatioДокумент47 страницFunctional Rehabilitation of Low Back Pain With Core StabilizatioEnyaw DroffatsОценок пока нет
- Anatomy of The FootДокумент17 страницAnatomy of The FootBlake BoggenpoelОценок пока нет
- Podiatry Dry NeedlingДокумент83 страницыPodiatry Dry NeedlingEnyaw Droffats100% (1)
- Myofascial PainДокумент8 страницMyofascial PainEnyaw Droffats100% (1)
- Back ExercisesДокумент1 страницаBack ExercisesEnyaw DroffatsОценок пока нет
- Myofascial PainДокумент8 страницMyofascial PainEnyaw Droffats100% (1)
- Deep Muscle Therapy 1 Intro 06Документ33 страницыDeep Muscle Therapy 1 Intro 06Enyaw DroffatsОценок пока нет
- Musculoskeletal Function - An Anatomy & KinesiologyДокумент135 страницMusculoskeletal Function - An Anatomy & KinesiologyEnyaw DroffatsОценок пока нет
- Joint BreakingДокумент18 страницJoint BreakingEnyaw DroffatsОценок пока нет
- Anatomy and Aikido - Perceptual and Motor SkillsДокумент24 страницыAnatomy and Aikido - Perceptual and Motor SkillsEnyaw Droffats100% (1)
- C27 and C32 Generator With EMCP4.2 Electrical SystemДокумент2 страницыC27 and C32 Generator With EMCP4.2 Electrical SystemAngel BernacheaОценок пока нет
- Orbeez Sorting and Patterns Learning ExperienceДокумент5 страницOrbeez Sorting and Patterns Learning Experienceapi-349800041Оценок пока нет
- Concept Deck de BosBoerderij - Dec2023Документ32 страницыConcept Deck de BosBoerderij - Dec2023Bruna San RomanОценок пока нет
- Metamath: A Computer Language For Mathematical ProofsДокумент247 страницMetamath: A Computer Language For Mathematical ProofsJohn DoeОценок пока нет
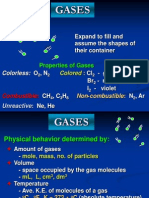
- Properties and Behavior of GasesДокумент34 страницыProperties and Behavior of GasesPaul Jeremiah Serrano NarvaezОценок пока нет
- Tie Technology DK SKДокумент32 страницыTie Technology DK SKVladimir PleșcaОценок пока нет
- She Walks in BeautyДокумент6 страницShe Walks in Beautyksdnc100% (1)
- Theories & Models of LearningДокумент33 страницыTheories & Models of LearningAna Paulina Suárez CervantesОценок пока нет
- AmpConectorsExtracto PDFДокумент5 страницAmpConectorsExtracto PDFAdrian AvilesОценок пока нет
- Lesson Plan For DemoДокумент7 страницLesson Plan For DemoShiela Tecson GamayonОценок пока нет
- Lali The Sun Also Rises Final PaperДокумент4 страницыLali The Sun Also Rises Final PaperDaniel AdamsОценок пока нет
- 2015 StoneAge - LowresДокумент51 страница2015 StoneAge - LowresAZLAN ABDULLAIОценок пока нет
- En GBДокумент4 страницыEn GBahmedОценок пока нет
- Key concepts in biology examДокумент19 страницKey concepts in biology examAditya RaiОценок пока нет
- Chapter 7Документ22 страницыChapter 7one loveОценок пока нет
- Rebecca A. Endaya Beed-Iii Art Education: ExploreДокумент5 страницRebecca A. Endaya Beed-Iii Art Education: ExploreBhecca Endaya0% (1)
- Record of Appropriations and Obligations: TotalДокумент1 страницаRecord of Appropriations and Obligations: TotaljomarОценок пока нет
- Educational PlanningДокумент20 страницEducational PlanningedelynОценок пока нет
- 53 Midas-Xr Analysis enДокумент33 страницы53 Midas-Xr Analysis encristiОценок пока нет
- Hunch or Reason?: Reading File 11Документ2 страницыHunch or Reason?: Reading File 11georgiana dinuОценок пока нет
- Topic 2Документ6 страницTopic 2Vince Diza SaguidОценок пока нет
- Mr. Sanjeev Nanda - Devoted Son and GrandsonДокумент1 страницаMr. Sanjeev Nanda - Devoted Son and GrandsonSanjeev NandaОценок пока нет
- Models of Collaboration Between Education and ServicesДокумент17 страницModels of Collaboration Between Education and ServicesSimran Josan100% (3)
- ICT Backup Procedure PolicyДокумент8 страницICT Backup Procedure PolicySultan BatoorОценок пока нет
- Current Electricity O LevelДокумент59 страницCurrent Electricity O LevelNoah OkitoiОценок пока нет
- M and S - Capstone Marketing Across Cultures Fons TrompenaarsДокумент398 страницM and S - Capstone Marketing Across Cultures Fons TrompenaarsBof BeosОценок пока нет
- QUARMEN Prerequisites - SEM1Документ12 страницQUARMEN Prerequisites - SEM1Valérie NguyenОценок пока нет
- HRBPДокумент8 страницHRBPPriscilia KarinaОценок пока нет
- Analyzing Visual TextsДокумент4 страницыAnalyzing Visual Textsapi-582845240Оценок пока нет
- QF-16 Security ProceduresДокумент55 страницQF-16 Security Proceduresmaruka33Оценок пока нет