Вам также может понравиться
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Principles of YogaДокумент8 страницPrinciples of YogaMahendra100% (2)
- CVS Case ProformaДокумент2 страницыCVS Case ProformaRiyaSingh100% (1)
- DesenteryДокумент3 страницыDesenteryAby Gift AnnОценок пока нет
- NCM 116 - RLE Activity#1 - VALDEZ PDFДокумент6 страницNCM 116 - RLE Activity#1 - VALDEZ PDFDexel Lorren ValdezОценок пока нет
- Pediatric Cutaneus of Larva MigransДокумент12 страницPediatric Cutaneus of Larva MigransSarah M PanjaitanОценок пока нет
- Pathophysiology Dyslipidemia PDFДокумент9 страницPathophysiology Dyslipidemia PDFtiffa07110% (1)
- ATYPICAL Pneumonias Caused by Legionella Pneumophila, Chlamydophila Pneumoniae and Mycoplasma Pneumonia PDFДокумент8 страницATYPICAL Pneumonias Caused by Legionella Pneumophila, Chlamydophila Pneumoniae and Mycoplasma Pneumonia PDFShelyAzradОценок пока нет
- Compile Nclex - RN Questions and AnswersДокумент17 страницCompile Nclex - RN Questions and Answerseric0% (1)
- Herpes Zoster Ophthalmicus: Ophthalmic PearlsДокумент3 страницыHerpes Zoster Ophthalmicus: Ophthalmic Pearlssiti rumaisaОценок пока нет
- Medical Nutrition Therapy 4 Cardiovascular Disease April 2012-RevisiДокумент66 страницMedical Nutrition Therapy 4 Cardiovascular Disease April 2012-RevisiFachri Ihsan100% (1)
- MCU 2021 The Ventilator Book 3rd EditionДокумент280 страницMCU 2021 The Ventilator Book 3rd EditionAlvaro Estupiñan100% (2)
- Espiro Alberto Dauce: The Impact of COVID-19 On Education in MozambiqueДокумент12 страницEspiro Alberto Dauce: The Impact of COVID-19 On Education in MozambiqueJustino Antonio Ernesto MartinhoОценок пока нет
- MBBS Pathology 3ed Semester Questions 2019-20Документ11 страницMBBS Pathology 3ed Semester Questions 2019-20RAJDEEP DASОценок пока нет
- UNIVERSITY OF MEDICAL SCIENCES"REZONANCA"-Halil Ajvazi/Ophthalmology/Prishtina/Republic of KosovaДокумент98 страницUNIVERSITY OF MEDICAL SCIENCES"REZONANCA"-Halil Ajvazi/Ophthalmology/Prishtina/Republic of KosovaHALIL Z.AJVAZI100% (1)
- Core V - Cardiovascular CoreДокумент35 страницCore V - Cardiovascular CoreMatthew LeiОценок пока нет
- CWU OrthopedicsДокумент6 страницCWU OrthopedicsSana Anam JahanОценок пока нет
- Radiology DVTДокумент90 страницRadiology DVTDhruv KushwahaОценок пока нет
- Wells - Oral - PathologyДокумент14 страницWells - Oral - PathologythesabarmoОценок пока нет
- Febrile Seizure PDFДокумент14 страницFebrile Seizure PDFgetnaniОценок пока нет
- Catatonia Revived. A Unique Syndrome UpdatedДокумент10 страницCatatonia Revived. A Unique Syndrome UpdatedElisa PavezОценок пока нет
- Gestational Diabetes Mellitus: A Harbinger of The Vicious Cycle of DiabetesДокумент21 страницаGestational Diabetes Mellitus: A Harbinger of The Vicious Cycle of DiabetesEmma Lyn SantosОценок пока нет
- Unit 11 Role of Fungi in Human Welfare: ObjectivesДокумент12 страницUnit 11 Role of Fungi in Human Welfare: Objectivessivaram888Оценок пока нет
- D Kerala PSC Staff Nurse Grade 2 Model Questions Part 4 - Kerala PSC QuestionsДокумент6 страницD Kerala PSC Staff Nurse Grade 2 Model Questions Part 4 - Kerala PSC QuestionsMrudula SureshОценок пока нет
- Guidelines For Preventing Foodborne Illness in SchoolДокумент27 страницGuidelines For Preventing Foodborne Illness in Schoolnaveed_akbar_2Оценок пока нет
- NURSING CARE PLAN - Liver CirrhosisДокумент2 страницыNURSING CARE PLAN - Liver Cirrhosisderic100% (27)
- Medical CertificateДокумент1 страницаMedical Certificatetri rahmawatiОценок пока нет
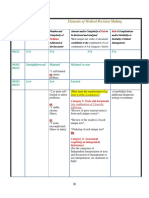
- 3-Level of MDMДокумент3 страницы3-Level of MDMmedical codingОценок пока нет
- More Simply Human - On The Universality of Madness (Nancy McWilliams)Документ11 страницMore Simply Human - On The Universality of Madness (Nancy McWilliams)Anastasiya PlohihОценок пока нет
- Organic Mental Disorders: DR - Deddy Soestiantoro SP - KJ M.KesДокумент20 страницOrganic Mental Disorders: DR - Deddy Soestiantoro SP - KJ M.KesBilly DarismaОценок пока нет
- Rule 23Документ5 страницRule 23everydaylarae100% (1)