Вам также может понравиться
- Lower Extremity NeuroДокумент3 страницыLower Extremity Neuroapi-238049665Оценок пока нет
- The Ankle and FootДокумент10 страницThe Ankle and Footapi-238049665Оценок пока нет
- HandДокумент5 страницHandapi-238049665Оценок пока нет
- Conciousness Cerebrum CN and PnsДокумент8 страницConciousness Cerebrum CN and Pnsapi-238049665Оценок пока нет
- Respi DrugsДокумент1 страницаRespi Drugsapi-238049665Оценок пока нет
- TSP and RibsДокумент7 страницTSP and Ribsapi-238049665Оценок пока нет
- L SpineДокумент13 страницL Spineapi-238049665Оценок пока нет
- Haematologic DiseaseДокумент3 страницыHaematologic Diseaseapi-238049665Оценок пока нет
- The Elbow ComplexДокумент6 страницThe Elbow Complexapi-238049665Оценок пока нет
- Shoulder ComplexДокумент7 страницShoulder Complexapi-238049665Оценок пока нет
- PorosispeniaparathyДокумент2 страницыPorosispeniaparathyapi-238049665Оценок пока нет
- Cvs DrugsДокумент4 страницыCvs Drugsapi-238049665Оценок пока нет
- CSPДокумент9 страницCSPapi-238049665Оценок пока нет
- Fibroids PresentationДокумент6 страницFibroids Presentationapi-238049665Оценок пока нет
- Ha Dizzines TinnitusДокумент9 страницHa Dizzines Tinnitusapi-238049665Оценок пока нет
- Gitendocrine DrugsДокумент4 страницыGitendocrine Drugsapi-238049665Оценок пока нет
- Upper ExtremityДокумент3 страницыUpper Extremityapi-238049665Оценок пока нет
- The Ankle and FootДокумент9 страницThe Ankle and Footapi-238049665Оценок пока нет
- LPTДокумент9 страницLPTapi-238049665Оценок пока нет
- Carpal Tunnel Syndrome PresentationДокумент4 страницыCarpal Tunnel Syndrome Presentationapi-238049665Оценок пока нет
- The Elbow ComplexДокумент6 страницThe Elbow Complexapi-238049665Оценок пока нет
- HandДокумент5 страницHandapi-238049665Оценок пока нет
- Shoulder ComplexДокумент7 страницShoulder Complexapi-238049665Оценок пока нет
- Lower Extremity NeuroДокумент3 страницыLower Extremity Neuroapi-238049665Оценок пока нет
- Respiratory Exam1Документ12 страницRespiratory Exam1api-238049665Оценок пока нет
- L SpineДокумент10 страницL Spineapi-238049665Оценок пока нет
- CSPДокумент9 страницCSPapi-238049665Оценок пока нет
- TSP and RibsДокумент7 страницTSP and Ribsapi-238049665Оценок пока нет
- The Hip: FunctionsДокумент7 страницThe Hip: Functionsapi-238049665Оценок пока нет
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5782)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- DLP Science Week 6 Day 5Документ3 страницыDLP Science Week 6 Day 5John Carlo DinglasanОценок пока нет
- Assignment 1 Systems Analysis - EME5601Документ7 страницAssignment 1 Systems Analysis - EME5601Travis GrantОценок пока нет
- RUDDER PLATING DIAGRAMДокумент1 страницаRUDDER PLATING DIAGRAMMuhammad Ilham AlfiansyahОценок пока нет
- Surface-Based Transport Model For Mixed-Size Sediment: Peter R. Wilcock, M.ASCE, and Joanna C. CroweДокумент9 страницSurface-Based Transport Model For Mixed-Size Sediment: Peter R. Wilcock, M.ASCE, and Joanna C. CroweEdwinОценок пока нет
- Hanoi 2023 Peoples Picks AwardsДокумент113 страницHanoi 2023 Peoples Picks AwardsNguyen Anh VuОценок пока нет
- Explore the Precambrian EraДокумент3 страницыExplore the Precambrian EraArjay CarolinoОценок пока нет
- Wattgate 381 Audio Grade Duplex Socket - y CableДокумент20 страницWattgate 381 Audio Grade Duplex Socket - y Cableapi-11530725100% (1)
- Fischer Carbene Complexes in Organic SynthesisДокумент9 страницFischer Carbene Complexes in Organic SynthesisNorah AltayyarОценок пока нет
- RenderingДокумент6 страницRenderingJuno PajelОценок пока нет
- Chapter 6 Exercises (Bonds & Interest)Документ2 страницыChapter 6 Exercises (Bonds & Interest)Shaheera SuhaimiОценок пока нет
- An Antarasiddhi, The First Independent Treatise: Masahiro InamiДокумент19 страницAn Antarasiddhi, The First Independent Treatise: Masahiro InamiFengfeifei2018Оценок пока нет
- Galaxy NanoporeДокумент11 страницGalaxy NanoporeDeborah ShirleenОценок пока нет
- TATA Gluco PDFДокумент5 страницTATA Gluco PDFsidharth dasОценок пока нет
- 3ixso2idq334tonwmfhk0rrcДокумент2 страницы3ixso2idq334tonwmfhk0rrcrishikeshraj2021Оценок пока нет
- Lynn Waterhouse - Critique On Multiple IntelligenceДокумент20 страницLynn Waterhouse - Critique On Multiple IntelligencenkrontirОценок пока нет
- Esquematicos CaterpillarДокумент9 страницEsquematicos Caterpillarluis alberto rodriguez100% (1)
- CQ B TECHNIQUESДокумент37 страницCQ B TECHNIQUESeddie6355100% (3)
- Technical Manual: Package Air Conditioner Rooftop - Cooling Only (50Hz)Документ56 страницTechnical Manual: Package Air Conditioner Rooftop - Cooling Only (50Hz)Im Chinith100% (1)
- 066 LW Tensile Tester v2.0 PDFДокумент4 страницы066 LW Tensile Tester v2.0 PDFMarkusОценок пока нет
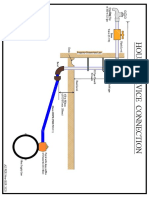
- House Service Connection NEW BSR 2020-1Документ1 страницаHouse Service Connection NEW BSR 2020-1Deshraj BairwaОценок пока нет
- ASTM D 2726 - 05a Standard Test Method For Bulk Specific Gravity and DensityДокумент4 страницыASTM D 2726 - 05a Standard Test Method For Bulk Specific Gravity and DensityAzlan AbdОценок пока нет
- Micro Teaching Lesson Plan in ScienceДокумент4 страницыMicro Teaching Lesson Plan in ScienceAB LoveriaОценок пока нет
- AC Circuit 2 (Three-Phase)Документ2 страницыAC Circuit 2 (Three-Phase)marlon desaculaОценок пока нет
- Common Sense Renewed R. C. ChristianДокумент276 страницCommon Sense Renewed R. C. Christianwarhed76100% (3)
- Presentation 1Документ26 страницPresentation 1Vaibhav Hireraddi100% (1)
- 7 Must Have Equipment Items For Your Church Safety TeamДокумент7 страниц7 Must Have Equipment Items For Your Church Safety TeamhmareidОценок пока нет
- PV Elite ResultДокумент18 страницPV Elite ResultVeny MartianiОценок пока нет
- Network 18Документ44 страницыNetwork 18Ashok ThakurОценок пока нет
- SWZ Upgrade Points 062022Документ19 страницSWZ Upgrade Points 062022IcyAviatorОценок пока нет