Академический Документы
Профессиональный Документы
Культура Документы
Prolonge Jaundice
Загружено:
vorezАвторское право
Доступные форматы
Поделиться этим документом
Поделиться или встроить документ
Этот документ был вам полезен?
Это неприемлемый материал?
Пожаловаться на этот документАвторское право:
Доступные форматы
Prolonge Jaundice
Загружено:
vorezАвторское право:
Доступные форматы
REVIEW ARTICLE
Prolonged neonatal jaundice: When to worry and what to do
Susan M Gilmour MD FRCPC
SM Gilmour. Prolonged neonatal jaundice: When to worry and what to do. Paediatr Child Health 2004;9(10):700-704.
Neonatal jaundice persisting beyond 14 days of age is a common clinical scenario. The vast majority of affected children have a benign unconjugated hyperbilirubinemia, but included in this clinical presentation is a group of neonates with conjugated hyperbilirubinemia and liver disease. Early identification of liver disease improves the infants outcome, especially for those with extrahepatic biliary atresia. The present paper reviews the approach to the neonate with prolonged jaundice, including clinical presentation, when to proceed with initial investigations, timing of referral, further investigations and management, and provides an overview of the more common causes of neonatal cholestatic liver disease.
La jaunisse nonatale prolonge : Quand sinquiter et quoi faire
La jaunisse nonatale qui persiste plus de 14 jours de vie constitue un scnario clinique courant. La majorit des enfants atteints souffrent dhyperbilirubinmie bnigne non conjugue, mais cette prsentation clinique inclut galement un groupe de nouveau-ns atteints dhyperbilirubinmie conjugue et de maladie hpatique. Un dpistage prcoce de la maladie hpatique amliore lissue du nourrisson, surtout sil souffre datrsie extrahpatique des voies biliaires. Le prsent examen permet danalyser la dmarche adopter lgard du nouveau-n atteint dune jaunisse prolonge, y compris sa prsentation clinique, le moment de procder aux premiers examens, le moment convenable pour procder laiguillage, les examens plus approfondis et la prise en charge, et fournit un aperu des causes les plus courantes de maladie hpatique cholestatique nonatale.
Key Words: Cholestatic liver disease; Neonatal jaundice
ersistent jaundice in the neonate is defined as jaundice that lasts longer than 14 to 21 days (1). It can occur in up to 15% of all newborns (2). The vast majority of these neonates have benign unconjugated hyperbilirubinemia but one in 2500 live births has cholestatic liver disease (3). The difficult task facing primary care providers is discriminating between serious conjugated hyperbilirubinemia and benign unconjugated jaundice because in the early stage, the infants can look very well except for their jaundice. Early identification of infants with cholestatic liver disease is critical so that a correct diagnosis is made and the appropriate therapy is instituted. The most compelling evidence for the importance of early detection is the condition of extrahepatic biliary atresia. It is the single most common cause of neonatal liver disease (4). Without therapy, its natural course is very poor, with less than 10% survival by the third year (5). Survival and outcome are improved with a Kasai portoenterostomy to restore bile drainage. The most important predictor of success is early age at operation (5), preferably 60 days of age or younger (6). Exploring all causes of the diagnostic and management dilemma of neonatal jaundice is beyond the scope of this article. Rather, the article will focus on the issue of the jaundiced infant in an outpatient setting, including initial management, interpretation of findings and timing of refer-
ral, as well as review some of the more common causes of cholestatic liver disease. PRESENTATION Clinically, most patients with cholestatic liver disease have jaundice, dark urine and pale stools, but otherwise look well. The presence of pale stools is a sensitive marker for liver disease, but parental reports of the history of stool colour may be misleading because the stool colour may be influenced by oral intake. Infants with severe liver disease may also present with encephalopathy, which might be difficult to diagnose in the neonatal period because it may manifest with nonspecific poor feeding and sleep disturbances. Another presentation of severe liver disease is bleeding and bruising due to vitamin K deficiency. Far less common is the presentation of seizures, either from hypocalcemia secondary to vitamin D deficiency or from hypoglycemia. A thorough physical examination may provide evidence of cholestatic liver disease and its underlying etiology. Some helpful features may include dysmorphic faces (Alagilles syndrome), evidence of congenital heart disease (Alagilles syndrome, biliary atresia), an abdominal mass (choledochal cyst, tumour), hepatomegaly/splenomegaly (found with obstruction, inflammation, a storage disorder or tumour), failure to thrive and an abnormal respiratory examination (cystic fibrosis). In addition, the neuromuscular examination
Division of Pediatric Gastroenterology/Nutrition, Stollery Childrens Hospital, University of Alberta, Edmonton, Alberta Correspondence: Dr S Gilmour, Division of Pediatric Gastroenterology/Nutrition, Stollery Childrens Hospital 2C3 WMC, University of Alberta, Edmonton, Alberta T6G 2R7. Telephone 780-407-3339, fax 780-407-3507, e-mail sgilmour@cha.ab.ca 700
2004 Pulsus Group Inc. All rights reserved
Paediatr Child Health Vol 9 No 10 December 2004
Prolonged neonatal jaundice
TABLE 1 Differential diagnosis of neonatal cholestatic liver disorders
Structural Extrahepatic biliary atresia Choledochal cyst Carolis syndrome Choledocholithiasis Alagilles syndrome Nonsyndromic bile duct paucity Undersized extrahepatic biliary system (biliary hypoplasia) Neonatal sclerosing cholangitis Infection Viral - Cytomegalovirus - Herpes simplex - Adenovirus - Enterovirus - Parvovirus B19 - Hepatitis B virus Bacterial infection (sepsis or remote from liver [eg, urinary tract infection]) Toxoplasmosis Syphilis Metabolic Alpha-1-antitrypsin deficiency Galactosemia Tyrosinemia Hereditary fructose intolerance Glycogen storage disease type IV Lipid storage disease - Niemann-Pick disease type A - Niemann-Pick disease type C - Gauchers disease - Wolmans disease Mitochondrial enzymopathies (including fatty acid oxidation disorders) Peroxisomal disorders (eg, Zellweger syndrome) Bile acid synthesis disorders Progressive familial intrahepatic cholestasis syndromes - FIC-1 protein deficiency (PFIC 1) - Bile salt export pump deficiency (PFIC 2) - MDR3 protein deficiency (PFIC 3) North American Indian familial cholestasis Urea cycle defects Genetic Cystic fibrosis Trisomy 21 Trisomy 18 Neoplastic Neuroblastoma Hepatoblastoma Histiocytosis X Toxic Drug induced Total parenteral nutrition Endocrine Panhypopituitarism Hypothyroidism Immune Neonatal lupus erythematosus Vascular Budd-Chiari syndrome Congestive heart failure Hepatic hemagiomatosis Idiopathic
TABLE 2 Initial investigations for conjugated hyperbilirubinemia
Blood Liver panel: aspartate aminotransferase, alanine aminotransferase, alkaline phosphatase, gamma-glutamyl transpeptidase, total bilirubin, conjugated bilirubin and albumin Coagulation studies (prothrombin time/international normalized ratio, partial thromboplastin time) Complete blood count and differential with smear Toxoplasmosis, other infections, rubella, Cytomegalovirus infection and herpes simplex (TORCH) serology Blood culture Hepatitis B surface antigen Glucose/serum lactate/serum amino acids/ammonia Thyroxine, thyroid-stimulating hormone Iron studies, ferritin Galactosemia screen Urine Reducing substances Organic acids Bacterial culture Urine Cytomegalovirus (positive result before four weeks of age is highly suggestive of congenital Cytomegalovirus) Imaging Abdominal ultrasound (evaluate for mass, choledochal cyst, small gallbladder, triangular cord sign)
may reveal hypotonia or abnormal reflexes (as with mitochondrial disorders and vitamin E deficiency). INITIAL EVALUATION Because the differential diagnosis of neonatal conjugated hyperbilirubinemia is very broad (Table 1), it is important to have a structured approach to its investigation. The most important investigation is to determine whether the infant with prolonged jaundice has liver disease or benign jaundice. The timing of initial investigations should occur between two to four weeks of age (1,6,7). The fractionation of the total serum bilirubin into its conjugated (direct) and unconjugated (indirect) components is the most important initial investigation. The bilirubin may be reported as indirect/direct or conjugated/unconjugated bilirubin, depending on the method used in the laboratory. Definitions of elevated conjugated hyperbilirubinemia may be based on absolute values in the context of a predominantly unconjugated hyperbilirubinemia (more than 35 mol/L) or the percentage of total bilirubin (more than 15%) (8), but for practical purposes, and because of laboratory variation, any elevation of conjugated bilirubin should be considered abnormal, and warrants further investigations and a referral to a paediatric gastroenterologist. Initial investigations that may be ordered by the primary care physician are outlined in Table 2. It is important to rule out conditions that require immediate treatment, such as infection, inborn errors of metabolism, hypothyroidism and identification of patients with liver failure as evidenced by hepatic synthetic dysfunction. After these potential
701
Paediatr Child Health Vol 9 No 10 December 2004
Gilmour
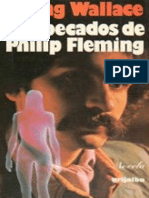
Conjugated hyperbilirubinemia
Initial investigations (Table 2 )
Other Investigations Sweat chloride Alpha-1-antitrypsin phenotype Urine bile acid metabolites Chest X-ray
Abdominal ultrasound
Choledochal cyst Dilated biliary tree
Normal or small gallbladder
Surgery
Hepatobiliary scan
Liver biopsy
Biliary hypoplasia
Neonatal hepatitis
Bile duct proliferation Bile plugs
Alagilles syndrome Ophthalmology Echocardiogram Genetic counselling
Excretion hepatobiliary scan
No excretion hepatobiliary scan
No excretion hepatobiliary scan
Medical therapy
Follow with medical therapy until 8 weeks
Laparotomy and intraoperative cholangiogram
No clinical improvement or worse
May rebiopsy, rescan or laparotomy to rule out extrahepatic biliary atresia
Figure 1) Flow chart for the investigation and management of conjugated hyperbilirubinemia
diagnoses have been eliminated, the most important differential diagnosis is biliary atresia. FURTHER INVESTIGATIONS The approach to the diagnostic evaluation and management of the infant with conjugated hyperbilirubinemia is outlined in Figure 1.
702
Abdominal ultrasound Abdominal ultrasound may be performed before and/or after referral to paediatric gastroenterology. It is a very sensitive method for diagnosing choledochal cysts and for detailing the anatomical abnormalities associated with the embryonic form of extrahepatic biliary atresia (midline liver, polysplenia or asplenia). While a small or absent gallbladder
Paediatr Child Health Vol 9 No 10 December 2004
Prolonged neonatal jaundice
is suggestive of extrahepatic biliary atresia, it is not diagnostic. Although extrahepatic biliary atresia is an obstructive process, it is important to note that bile duct dilation is not ordinarily a feature of biliary atresia. Some literature (9) suggests that the triangular cord sign (an echogenic area in the porta hepatis) is very specific for biliary atresia, although the demonstration of this finding is very operatordependent, limiting its widespread use (9). Hepatobiliary scanning The nuclear medicine imaging procedure of hepatobiliary scanning uses technetium-labelled iminodiacetic derivatives. Infants should receive three to five days of phenobarbital (5 mg/kg/day) to promote hepatocellular uptake of the tracer. Serial images are obtained evaluating hepatocellular uptake and biliary excretion into the small intestine. Hepatobiliary scanning is almost 100% sensitive for extrahepatic biliary atresia because the excretion of tracer into the small bowel almost always rules out biliary atresia. Unfortunately, a nondraining scan is not specific and it can have many different etiologies (10). Although the test has poor specificity, it is useful when the liver biopsy is nondiagnostic. Liver biopsy Liver biopsy is the most informative investigation in the evaluation of neonatal conjugated hyperbilirubinemia, with many centres reporting over 90% accuracy for biliary atresia (1). Some histological findings include bile ductular proliferation, bile plugging and portal fibrosis in biliary atresia, parenchymal inflammatory infiltrate and giant cell transformation in neonatal hepatitis, and portal duct hypoplasia with Alagilles syndrome. Further immunostaining, histochemistry and electron microscopy can assist in the diagnosis of other disorders, such as alpha-1-antitrypsin deficiency and some storage disorders. SPECIFIC DISORDERS On completion of the investigations outlined in Table 2 and Figure 1, the etiology of neonatal conjugated hyperbilirubinemia tends to fall into one of five groups: biliary atresia (30%), idiopathic neonatal hepatitis (25%), intrahepatic cholestasis (including Alagilles syndrome) (15%) and a collection of infectious and rare disorders (11,12) (approximately 30%). Extrahepatic biliary atresia Extrahepatic biliary atresia is the progressive obliteration of the extrahepatic bile ducts that leads to fibrosis and damage of the intrahepatic bile ducts. The incidence is 1:8000 to 1:15,000 live births (7). It is the most common disease requiring liver transplantation in childhood. The cause of the inflammation and biliary destruction is unknown, although many mechanisms have been implicated, including immunological, viral (Cytomegalovirus [CMV] and Reovirus type 3), ischemic or genetic mechanisms, as well as toxic bile acids (8,13). Extrahepatic
Paediatr Child Health Vol 9 No 10 December 2004
biliary atresia is usually classified into two phenotypes. The embryonic form is found in 10% to 20% of patients and is associated with other anomalies, including splenic malformation, abnormalities of the portal vein and inferior vena cava, situs inversus and congenital heart disease. The perinatal form is by far the most common. These patients typically present with a history of being well at birth and for their first few weeks, with jaundice appearing after the first week of life. The gold standard for diagnosis of extrahepatic biliary atresia is laparotomy with an intraoperative cholangiogram. The treatment is a Kasai portoenterostomy in which the atretic extrahepatic tissue is removed and a Roux-en-Y jejunal loop is anastomosed to the hilum where patent bile ducts have been dissected. The success of this operation is greatly influenced by the age of the child at the time of surgery, with the greatest success seen when surgery is performed before 60 days of age (5,6). Infections CMV is the most common cause of congenital infection, and 60% to 80% of symptomatic children can have hepatosplenomegaly and jaundice (7). CMV affects the central nervous system, and affected patients may present with microcephaly, intracranial calcifications and chorioretinitis. CMV rarely results in cirrhosis and chronic liver disease. Other TORCH infections (Toxoplasmosis, Other infections, Rubella, Cytomegalovirus infection and Herpes simplex) may have hepatosplenomegaly and jaundice as part of the congenital infection. Hepatotropic viruses (hepatitis A, B and C) rarely cause neonatal jaundice. Hepatitis B and C are vertically transmitted and are usually subclinical, although hepatitis B may cause a neonatal hepatitis. Conjugated hyperbilirubinemia may occur with bacterial sepsis, especially urinary tract infection (14), and this must be ruled out with the initial investigations. Alagilles syndrome Alagilles syndrome has the feature of portal bile duct hypoplasia. The genetic basis for this syndrome is a mutation in the jagged 1 gene on chromosome 20p (15). Alagilles syndrome is an autosomal dominant disorder with variable penetrance and up to 50% of patients show new mutations. The syndrome has variable penetrance with heterogeneity of clinical manifestations. There are five major clinical features: chronic cholestasis; faces with a broad forehead, recessed eyes and a small chin; vertebral anomalies, including butterfly vertebrae; cardiac anomalies (most commonly peripheral pulmonary stenosis); and ocular abnormalities, including posterior embryotoxon.
703
Gilmour
Other clinical findings include renal abnormalities, developmental delay, growth retardation and vascular abnormalities. Infants usually present with neonatal cholestasis and the characteristic facies, although these may be difficult to recognize in the neonatal period. If children with the syndrome present with jaundice, the prognosis is that 50% will die or require a transplant by 10 years of age. Alpha-1-antitrypsin deficiency Alpha-1-antitrypsin deficiency is a common inherited cause of neonatal conjugated hyperbilirubinemia. It is a common protease inhibitor that is produced in hepatocytes. Approximately 1:2000 to 1:3000 individuals is homozygous for the Z mutation, and the ZZ phenotype is associated with neonatal liver disease and adult emphysema. Only 10% to 15% of infants with the ZZ phenotype will present with liver disease. The mechanism for the liver disease and why this minority of infants with the ZZ phenotype have jaundice are unclear. Liver disease seems to be related to hepatocyte accumulation of abnormal alpha-1-antitrypsin, along with inefficient excretion and some other undefined modifying factors (1). Idiopathic neonatal hepatitis After biliary atresia, the most common diagnosis is idiopathic neonatal hepatitis. Although no specific etiology can be demonstrated, these infants are more likely to have been born prematurely, be the product of a complicated pregnancy or have intrauterine growth retardation (1). The typical liver biopsy has hepatocyte giant cell transformation with inflammation. Prognosis is usually very good with 75% to 90% of cases resolved by one year (16). Predictors of poor prognosis include acholic stool, jaundice beyond six months, hepatomegaly, family history and a liver biopsy with severe inflammation (1). MANAGEMENT Intensive supportive therapy is required for all infants with cholestatic liver disease. Much of the management can be provided through a co-care model between the primary care physician and the paediatric gastroenterologist. One of the most important issues is nutritional support. Infants with cholestatic liver disease require high calorie diets with 120% to 150% of the estimated average requirements (17), and because of the lack of bile flow, they require an increased percentage of medium chain triglycerides. Infants must be followed closely, with adjustments of the caloric density and medium chain triglycerides content of the diet based on growth. Some infants may require nasogastric tube feeds to meet nutritional requirements. Fat-soluble vitamins must also be supplemented with aqueous preparations. Current recommendations are alpha-tocopherol (vitamin E) 25 IU/kg/day plus a twice daily dose of a liquid multivitamin supplement (eg, Poly-Vi-Sol, Mead Johnson and Company, USA) and 1 mg/day to 2 mg/day of vitamin K. The dose should be titrated based on
measurements of serum levels of vitamins A, D and E, and the results of coagulation studies. To promote bile flow and decrease the pruritus of cholestasis, ursodeoxycholic acid is used. The usual dose is 20 mg/kg/day. Further treatment of pruritus due to cholestasis may include cholestyramine to bind intestinal bile acids and prevent reabsorption, or rifampin (5 mg/kg/day to 10 mg/kg/day). The infants also require frequent monitoring by both their primary care physician and their paediatric gastroenterologist to assess for progression or resolution of their liver disease. Follow-up evaluation of physical findings, hepatic synthetic function, transaminases and evidence of portal hypertension are used to assess the progression of the liver disease. SUMMARY Early detection of infantile cholestatic liver disease is one of the greatest challenges facing the primary care provider. Although many infants are jaundiced beyond 14 days, it is imperative that they be investigated to facilitate early diagnosis and implementation of therapy. The most important measure in any infant persistently jaundiced beyond two weeks of age is the conjugated bilirubin level. Any elevation in bilirubin level should prompt investigations and immediate referral to a paediatric gastroenterologist.
REFERENCES
1. McKiernan PJ. Neonatal cholestasis. Semin Neonatol 2002;7:153-65. 2. Logan S, Stanton A. Screening for biliary atresia. Lancet 1993;342:256. 3. Roberts EA. The jaundiced baby. In: Kelly DA, ed. Disease of the Liver and Biliary System in Children, 1st edn. Oxford: Blackwell, 1999:11-45. 4. Knisely AS. Biliary atresia and its complications. Ann Clin Sci 1990;20:113-8. 5. Karrer FM, Lilly JR, Stewart BA, Hall RJ. Biliary atresia registry 1976-1989. J Pediatr Surg 1990;25:1076-81. 6. Hussein M, Howard ER, Mieli-Vergani G, Mowat AP. Jaundice at 14 days: Exclude biliary atresia. Arch Dis Child 1991;66:1177-9. 7. Roberts EA. Neonatal hepatitis syndrome. Semin Neonatol 2003;8:357-74. 8. Karpen SJ. Update on the etiologies and management of neonatal cholestasis. Clin Perinatol 2002;29:159-80. 9. Kotb MA, Kotb A, Sheba MF, et al. Evaluation of the triangular cord sign in the diagnosis of biliary atresia. Pediatrics 2001;108:416-20. 10. Gilmour SM, Hershkop M, Reifen R, Gilday D, Roberts EA. Outcome of hepatobiliary scanning in neonatal hepatitis syndrome. J Nucl Med 1997;38:1279-82. 11. Lichtman S, Guzman C, Moore DL, Weber SJ, Roberts EA. Mortality after percutaneous liver biopsy. Arch Dis Child 1987;62:901-4. 12. Balistreri WF. Neonatal cholestasis: Lessons from the past, issues for the future. Semin Liver 1987;7:61-6. 13. Tyler KL, Sokol RJ, Oberhaus SM, et al. Detection of reovirus RNA in hepatobiliary tissues from patients with extrahepatic biliary atresia and choledochal cysts. Hepatology 1998;27:1475-82. 14. Garcia FJ, Nager AL. Jaundice as an early diagnostic sign of urinary tract infection in infancy. Pediatrics 2002;109:846-51. 15. Spinner NB, Colliton RP, Crosnier C, Krantz ID, Hadchouel M, Meunier-Rotival M. Jagged 1 mutations in alagille syndrome. Hum Mutat 2001;17:18-33. 16. Suita S, Arima T, Ishii K, Yakabe S, Matsuo S. Fate of infants with neonatal hepatitis: Pediatric surgeons dilemma. J Pediatr Surg 1992;27:696-9. 17. Pierro A, Koletzko B, Carnielli V, et al. Resting energy expenditure is increased in infants and children with extrahepatic biliary atresia. J Pediatr Surg 1989;24:534-8.
704
Paediatr Child Health Vol 9 No 10 December 2004
Вам также может понравиться
- Test Initial Cls 8 Limba FrancezaДокумент4 страницыTest Initial Cls 8 Limba FrancezaMarinică Șchiopu100% (1)
- Mais Bon Baudry Mais BonДокумент27 страницMais Bon Baudry Mais Bonnr655321Оценок пока нет
- VSMДокумент33 страницыVSMsébastienОценок пока нет
- DCC#08 - Quand Les Lames Défient La MortДокумент36 страницDCC#08 - Quand Les Lames Défient La Mortzebulon100% (3)
- Texte - 4 Analyse Discours Sur La MisèreДокумент3 страницыTexte - 4 Analyse Discours Sur La MisèreFrancisco EmmanuelОценок пока нет
- Meurant - Romulus, Jumeau Et RoiДокумент29 страницMeurant - Romulus, Jumeau Et RoiMaurizio GallinaОценок пока нет
- Créer Un Nom de Marque Et Un Nom de DomaineДокумент162 страницыCréer Un Nom de Marque Et Un Nom de DomaineMoxaline100% (1)
- M1 PA 19-20 Génétique Quantitative ArboucheДокумент17 страницM1 PA 19-20 Génétique Quantitative ArboucheAbderrahim MalkiОценок пока нет
- Evaluation Diagnostique 4AM - Docx Version 1Документ3 страницыEvaluation Diagnostique 4AM - Docx Version 1saa diaОценок пока нет
- Dépliant FUPДокумент2 страницыDépliant FUProdolfoenjaОценок пока нет
- Le Systeme Nerveux Cours PDF 3Документ5 страницLe Systeme Nerveux Cours PDF 3HamidBenmansour100% (2)
- Gestionnaires! Du Leadership SVP CompétencesДокумент38 страницGestionnaires! Du Leadership SVP Compétencesmfagla100% (1)
- Une FemmeДокумент2 страницыUne FemmeManonОценок пока нет
- Bartolomé de Las Casas, OeuvresДокумент544 страницыBartolomé de Las Casas, OeuvresclassaraceОценок пока нет
- (Méthod'o.) Fragnière, Jean-Pierre-Comment Réussir Un Mémoire - Choisir Son Sujet, Gérer Son Temps, Savoir Rédiger-Dunod (DL 2016, 2016)Документ142 страницы(Méthod'o.) Fragnière, Jean-Pierre-Comment Réussir Un Mémoire - Choisir Son Sujet, Gérer Son Temps, Savoir Rédiger-Dunod (DL 2016, 2016)Jack Shepherd88% (8)
- Les Trente Trois Medaillons TrescasesДокумент35 страницLes Trente Trois Medaillons TrescasesRafael RodriguesОценок пока нет
- Chapitre 3 - Dyspnée AïgueДокумент47 страницChapitre 3 - Dyspnée AïguerachidОценок пока нет
- Partie 1 Enzymo FEV 12Документ61 страницаPartie 1 Enzymo FEV 12Limoune AliОценок пока нет
- Cours-Audit Comptable Et FinancierДокумент108 страницCours-Audit Comptable Et FinancierMessa Boualem100% (1)
- Champerret 2015Документ24 страницыChamperret 2015librairiechretien8174100% (1)
- Pierre de RonsardДокумент4 страницыPierre de RonsardMarianoJosuePintoColu0% (1)
- Gmv50 AsthmeДокумент2 страницыGmv50 AsthmekotonОценок пока нет
- Le Rejet de La Psycha 87264Документ8 страницLe Rejet de La Psycha 87264MinuxОценок пока нет
- Le Kit Du CampeurДокумент1 страницаLe Kit Du CampeurChristian LouaОценок пока нет
- Irving Wallace-Los Pecados de Philip Fleming 1Документ146 страницIrving Wallace-Los Pecados de Philip Fleming 1alterjack701Оценок пока нет
- Notes de Cours de Vih IIДокумент18 страницNotes de Cours de Vih IIRashidi YannickОценок пока нет
- Association Revue Française de Sociologie, Sciences Po University Press Revue Française de SociologieДокумент3 страницыAssociation Revue Française de Sociologie, Sciences Po University Press Revue Française de SociologieNAYRA LUNA MARGARITA CAPETILLO CAUTIVOОценок пока нет
- Systeme de Gestion de La SSTДокумент32 страницыSysteme de Gestion de La SSTDavid Njoungang100% (1)
- Edmond Cary - POUR UNE THÉORIE DE LA TRADUCTIONДокумент11 страницEdmond Cary - POUR UNE THÉORIE DE LA TRADUCTIONFernando ZemorОценок пока нет
- The Design of Everyday Things by Don Norman (En Français)Документ282 страницыThe Design of Everyday Things by Don Norman (En Français)Anderson KouadioОценок пока нет