Вам также может понравиться
- Ethinylestradiol 35mcg + Cyproterone Acetate 2mg (Diane - 35)Документ16 страницEthinylestradiol 35mcg + Cyproterone Acetate 2mg (Diane - 35)asdwasdОценок пока нет
- Ethinylestradiol Ph. Eur. 0.03mg + Desogestrel B.P 0.15mg (Microdiol)Документ19 страницEthinylestradiol Ph. Eur. 0.03mg + Desogestrel B.P 0.15mg (Microdiol)asdwasdОценок пока нет
- Select The Required Information: Professional Information Patient Information LeafletДокумент15 страницSelect The Required Information: Professional Information Patient Information LeafletInday RonangОценок пока нет
- Ethinylestradiol 0.02mg + Desogestrel 0.15mg (Mercilon)Документ19 страницEthinylestradiol 0.02mg + Desogestrel 0.15mg (Mercilon)ddandan_2Оценок пока нет
- Qlaira Film-Coated Tablets - Summary of Product Characteristics (SMPC) - (Emc)Документ1 страницаQlaira Film-Coated Tablets - Summary of Product Characteristics (SMPC) - (Emc)Rand KamalОценок пока нет
- DIENOGEST 2 MG + ETHINYLESTRADIOL 0.03 MG SPCДокумент22 страницыDIENOGEST 2 MG + ETHINYLESTRADIOL 0.03 MG SPCMaged BedeawyОценок пока нет
- SEO-Optimized Title for Qlair Film-Coated Tablets Product CharacteristicsДокумент26 страницSEO-Optimized Title for Qlair Film-Coated Tablets Product CharacteristicsasdwasdОценок пока нет
- Novelon Lite 28 InsertДокумент2 страницыNovelon Lite 28 InsertKhuub TeshОценок пока нет
- Ethinylestradiol As Betadex Calthrate 0.02mg + Drospirenone 3mg + Levomefolate Calcium 0.451mg (Yaz Plus)Документ24 страницыEthinylestradiol As Betadex Calthrate 0.02mg + Drospirenone 3mg + Levomefolate Calcium 0.451mg (Yaz Plus)ddandan_2Оценок пока нет
- Oralcontraceptives9 09Документ4 страницыOralcontraceptives9 09Patrick BatemanОценок пока нет
- Combined Oral Contraceptive Pill: Choice of Pill: For First Time UsersДокумент30 страницCombined Oral Contraceptive Pill: Choice of Pill: For First Time UsersMohammed Saad NabhanОценок пока нет
- DexamethasoneДокумент4 страницыDexamethasoneAfidz Azuddin HaziqОценок пока нет
- Duphaston DR 1410193172635 PDFДокумент8 страницDuphaston DR 1410193172635 PDFjoyce ramirezОценок пока нет
- DIANE-35: Registered Package InsertДокумент5 страницDIANE-35: Registered Package InsertTrisha HОценок пока нет
- Everything You Need to Know About the Birth Control Pill Yasmin PlusДокумент23 страницыEverything You Need to Know About the Birth Control Pill Yasmin Plusddandan_2Оценок пока нет
- Estradiol 1.5mg + Nomegestrol Acetate 2.5mg (Zoely)Документ17 страницEstradiol 1.5mg + Nomegestrol Acetate 2.5mg (Zoely)asdwasdОценок пока нет
- Oral Hormonal Contraceptive: BY Magdyabdelrahmanmohamed 2 0 1 5Документ36 страницOral Hormonal Contraceptive: BY Magdyabdelrahmanmohamed 2 0 1 5UdtjeVanDerJeykОценок пока нет
- Combined Pill - NHSДокумент1 страницаCombined Pill - NHSkgothatsoОценок пока нет
- Ethinylestradiol 0.03mg + Drospirenone 3mg (Yasmin)Документ18 страницEthinylestradiol 0.03mg + Drospirenone 3mg (Yasmin)asdwasdОценок пока нет
- Dosing of Ivermectin & Other TherapeuticsДокумент7 страницDosing of Ivermectin & Other TherapeuticsTom100% (1)
- Emcon 1Документ8 страницEmcon 1biswasjoyОценок пока нет
- Yaz Plus en PiДокумент16 страницYaz Plus en PiMookwane Mashabela (Mo)Оценок пока нет
- Diane 35 PM pt3 PDFДокумент11 страницDiane 35 PM pt3 PDFHum BlumОценок пока нет
- Diane 35 en PiДокумент5 страницDiane 35 en PiJay r SulanaОценок пока нет
- 23 Eqed 23Документ10 страниц23 Eqed 23Keanu PeraltaОценок пока нет
- Artikel Keluarga Berencana, Izzatul Ummah FhadillaДокумент6 страницArtikel Keluarga Berencana, Izzatul Ummah FhadillaAQFAL storyОценок пока нет
- Ceu Statement Missed PillsДокумент3 страницыCeu Statement Missed PillsDaisuke GatsuОценок пока нет
- Managing Patients With Chronic AnginaДокумент10 страницManaging Patients With Chronic Anginacindyfuller68Оценок пока нет
- 2011 MicrogynonДокумент16 страниц2011 MicrogynontaikucinglohОценок пока нет
- Xylocaine Jelly Cil enДокумент4 страницыXylocaine Jelly Cil enRavi KumarОценок пока нет
- Dmpa 5 25 11Документ5 страницDmpa 5 25 11samuel adelОценок пока нет
- Contraception and FertilityДокумент11 страницContraception and FertilityWil LesterОценок пока нет
- Yaz PiДокумент29 страницYaz Piluci_sylviaОценок пока нет
- Oral Contraceptives: Presented byДокумент24 страницыOral Contraceptives: Presented byfarmasi_hm100% (1)
- Safe and Effective ContraceptiveДокумент24 страницыSafe and Effective ContraceptiveHarly KabutОценок пока нет
- Summary of Product Characteristics 1. Name of The Medicinal ProductДокумент13 страницSummary of Product Characteristics 1. Name of The Medicinal Productddandan_2Оценок пока нет
- Patient Information Leaflet Sustac Tablets 2.6 MG and 6.4 MGДокумент2 страницыPatient Information Leaflet Sustac Tablets 2.6 MG and 6.4 MGayazkhan74434Оценок пока нет
- FAQ Drug Info - TirzepatideДокумент9 страницFAQ Drug Info - Tirzepatideraea.dobsonОценок пока нет
- Diane 35 PM en PDFДокумент44 страницыDiane 35 PM en PDFAhmad MuhlisinОценок пока нет
- 615e98e38e63c Duvadilan Drug StudyДокумент3 страницы615e98e38e63c Duvadilan Drug StudyKimОценок пока нет
- Case AnalysisДокумент2 страницыCase AnalysisYeng MangilitОценок пока нет
- Risperidone Drug StudyДокумент2 страницыRisperidone Drug StudyNajmah Saaban77% (13)
- Region 2 University of La Salette, Inc. Santiago City, IsabelaДокумент7 страницRegion 2 University of La Salette, Inc. Santiago City, IsabelaronronОценок пока нет
- Instructions For Taking The 28-Day Birth Control PillДокумент3 страницыInstructions For Taking The 28-Day Birth Control PillGenoviv LappayОценок пока нет
- Pharmacy Skills Ia - Training 2 Exercise 2 - Hypertensive Patient U21104008 2023 10 17 13 45 37Документ9 страницPharmacy Skills Ia - Training 2 Exercise 2 - Hypertensive Patient U21104008 2023 10 17 13 45 37Sara HajeerОценок пока нет
- QweasdДокумент4 страницыQweasdJude FabellareОценок пока нет
- ADHD Medication Chart 2004Документ4 страницыADHD Medication Chart 2004M PatrickОценок пока нет
- CMI GastrostopДокумент3 страницыCMI GastrostopAdi DharmawanОценок пока нет
- TamifluhcpДокумент3 страницыTamifluhcpDr-Dalya ShakirОценок пока нет
- DrugsДокумент61 страницаDrugsPrabir SahaОценок пока нет
- Drug Study (DR)Документ19 страницDrug Study (DR)09159054476Оценок пока нет
- 4 - Hormonal ContraceptivesДокумент109 страниц4 - Hormonal ContraceptivesNoskcire OremorОценок пока нет
- Standard Treatment Guidelines - HysterectomyДокумент3 страницыStandard Treatment Guidelines - Hysterectomydr_rajatjainОценок пока нет
- Stugeron ForteДокумент4 страницыStugeron ForteJemsMei Comparativo MensuradoОценок пока нет
- What Is DiclofenacДокумент58 страницWhat Is Diclofenacmercy foundation100% (2)
- Drug Study 1Документ10 страницDrug Study 1neeraj chauhanОценок пока нет
- Diabetes FBДокумент4 страницыDiabetes FBAbdullah Yeamin PeyalОценок пока нет
- MEDEXAДокумент7 страницMEDEXAhaharameshОценок пока нет
- Naplex Complete Study Outline A Topic-Wise Approach DiabetesОт EverandNaplex Complete Study Outline A Topic-Wise Approach DiabetesРейтинг: 4 из 5 звезд4/5 (2)
- Prefix and Suffix, Blok 1 Untad 2012Документ30 страницPrefix and Suffix, Blok 1 Untad 2012Mardatillah WiranataОценок пока нет
- Daftar Keterampilan Medis Skills Lab Kurikulum PBL 2002Документ1 страницаDaftar Keterampilan Medis Skills Lab Kurikulum PBL 2002Mardatillah WiranataОценок пока нет
- Laboratory Practice in PBLДокумент84 страницыLaboratory Practice in PBLMardatillah WiranataОценок пока нет
- Teknik Penulisan VancouverДокумент25 страницTeknik Penulisan VancouverMardatillah WiranataОценок пока нет
- 5 6 ContinuityCareДокумент15 страниц5 6 ContinuityCareMardatillah WiranataОценок пока нет
- Daftar Keterampilan Medis Skills Lab Kurikulum PBL 2002Документ1 страницаDaftar Keterampilan Medis Skills Lab Kurikulum PBL 2002Mardatillah WiranataОценок пока нет
- Blok 6 Final and Brainstorming AnsweredДокумент13 страницBlok 6 Final and Brainstorming AnsweredMardatillah WiranataОценок пока нет
- Vaginitis A Do LДокумент17 страницVaginitis A Do LMardatillah WiranataОценок пока нет
- Anatomy and Physiology of EarДокумент11 страницAnatomy and Physiology of EarAriguna WijayaОценок пока нет
- Barthel IndexДокумент1 страницаBarthel IndexChu Ai Reen50% (2)
- Verruca VulgarissssДокумент1 страницаVerruca VulgarissssMardatillah WiranataОценок пока нет
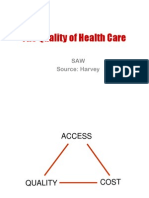
- The Quality of Health Care: SAW Source: HarveyДокумент43 страницыThe Quality of Health Care: SAW Source: HarveyMardatillah WiranataОценок пока нет
- Barthel Index (0-20)Документ2 страницыBarthel Index (0-20)Yessika Adelwin Natalia95% (19)
- Vulvo-Vaginitis Children : GatheringДокумент16 страницVulvo-Vaginitis Children : GatheringMardatillah WiranataОценок пока нет
- VaginitisДокумент2 страницыVaginitisMardatillah WiranataОценок пока нет
- 12 English in MedicineДокумент11 страниц12 English in MedicineIndra TandiОценок пока нет
- Digsetive BiochemistryДокумент10 страницDigsetive BiochemistryMardatillah WiranataОценок пока нет
- Urin 1Документ10 страницUrin 1Mardatillah WiranataОценок пока нет
- 1Документ11 страниц1Mardatillah WiranataОценок пока нет
- The Basic of Health Termsppt2007Документ24 страницыThe Basic of Health Termsppt2007Mardatillah WiranataОценок пока нет
- Ikm Okt2005 9Документ8 страницIkm Okt2005 9Wawan Masih The'cool'genkОценок пока нет
- Family Planning and Contrceptives For Midwifery StudentsДокумент190 страницFamily Planning and Contrceptives For Midwifery StudentsAbdusamed100% (1)
- Sexual Reproduction in Humans: Contraception: J. J. Marshall-Thompson Cape Biology Unit 1 20 APRIL, 2020Документ26 страницSexual Reproduction in Humans: Contraception: J. J. Marshall-Thompson Cape Biology Unit 1 20 APRIL, 2020Lavinia LaviaОценок пока нет
- Gonadal Hormones and InhibitorsДокумент14 страницGonadal Hormones and InhibitorsbluesumОценок пока нет
- EstrogenДокумент41 страницаEstrogenShanty ManekОценок пока нет
- A Pro-Life Pastoral HandbookДокумент109 страницA Pro-Life Pastoral HandbookCBCP for LifeОценок пока нет
- Modern Concept of Health and Primary Health CareДокумент213 страницModern Concept of Health and Primary Health CareMatt AndreyОценок пока нет
- CYL456: Chemistry of Life - An Introduction Biomolecules: LipidsДокумент45 страницCYL456: Chemistry of Life - An Introduction Biomolecules: LipidsMegraj MeenaОценок пока нет
- Artificial Birth ControlДокумент4 страницыArtificial Birth Controljessa tabanginОценок пока нет
- AOGD Bulletin November 2019Документ64 страницыAOGD Bulletin November 2019Kavitha NarayanaswamyОценок пока нет
- Intrauterine Drug Delivery SystemsДокумент32 страницыIntrauterine Drug Delivery SystemsAhmad ThantowiОценок пока нет
- 4 - Hormonal ContraceptivesДокумент109 страниц4 - Hormonal ContraceptivesNoskcire OremorОценок пока нет
- Chap2 Lesson 1-4Документ43 страницыChap2 Lesson 1-4Renalf Ezra BarbietoОценок пока нет
- DLL Mod.1 Part 3 3RD QRTR G10Документ7 страницDLL Mod.1 Part 3 3RD QRTR G10Kris Camille TanОценок пока нет
- Maternity Nursing I: Paul Jhon A. Vergara, RNДокумент40 страницMaternity Nursing I: Paul Jhon A. Vergara, RNPaul Jhon VergaraОценок пока нет
- Notes File - MergedДокумент99 страницNotes File - MergedMian. Shoaib.Оценок пока нет
- 08.04.20-AF, Unit-12, Family Wefare Programme, - Methods of contraception-8.04.20-ANДокумент65 страниц08.04.20-AF, Unit-12, Family Wefare Programme, - Methods of contraception-8.04.20-ANElakkiyaanu64 Elakkiyaanu64Оценок пока нет
- Advances in Reproductive EndocrinologyДокумент41 страницаAdvances in Reproductive Endocrinologyapi-3705046Оценок пока нет
- 2001 107 562-573 Donald E. Greydanus, Dilip R. Patel and Mary Ellen RimszaДокумент14 страниц2001 107 562-573 Donald E. Greydanus, Dilip R. Patel and Mary Ellen RimszaNurse AlzahraОценок пока нет
- Imle A 03 03 2015Документ82 страницыImle A 03 03 2015Moataz TrabehОценок пока нет
- Hormonal Contraception PDFДокумент28 страницHormonal Contraception PDFSini AbrahamОценок пока нет
- Paraphrase-RESEARCH FullДокумент46 страницParaphrase-RESEARCH Fullkeychain shopОценок пока нет
- Uts 2ND ExamДокумент2 страницыUts 2ND ExamJunzen Ralph YapОценок пока нет
- Obstetrics and GynecologyДокумент56 страницObstetrics and GynecologyAhmad MakhloufОценок пока нет
- Gynecology GY Emtyaz Quiz JordanДокумент40 страницGynecology GY Emtyaz Quiz JordanVicviclookThekingОценок пока нет
- Challenging Concepts in INTERVENTIONAL RADIOLOGY 1st EditionДокумент363 страницыChallenging Concepts in INTERVENTIONAL RADIOLOGY 1st EditionHisham Elkilaney100% (1)
- I. Objectives A. Content Standards: Monday Tuesday Wednesday Thursday FridayДокумент8 страницI. Objectives A. Content Standards: Monday Tuesday Wednesday Thursday FridayMaribel NayadОценок пока нет
- Aub Gyn PDFДокумент66 страницAub Gyn PDFArun RaviОценок пока нет
- Dysbiosis of The Human Oral Microbiome During The Menstrual Cycle and Vulnerability To The External Exposures of Smoking and Dietary SugarДокумент14 страницDysbiosis of The Human Oral Microbiome During The Menstrual Cycle and Vulnerability To The External Exposures of Smoking and Dietary SugarPaloma C. PeñaОценок пока нет
- Aqa Gcse Science Content BookДокумент216 страницAqa Gcse Science Content BookVincentBauzaОценок пока нет
- % Chapter 4: Hormonal Control of Reproductive CycleДокумент22 страницы% Chapter 4: Hormonal Control of Reproductive CycleK CОценок пока нет