Вам также может понравиться
- COMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideОт EverandCOMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideОценок пока нет
- Coarctation of The AortaДокумент7 страницCoarctation of The Aortamharz_astillo100% (1)
- Hypertension in PregnancyДокумент31 страницаHypertension in PregnancyradhabobbyОценок пока нет
- Tetralogy of FallotДокумент33 страницыTetralogy of FallotjeenaejyОценок пока нет
- 1 Fluid Volume Excess Chronic Renal Failure Nursing Care PlansДокумент3 страницы1 Fluid Volume Excess Chronic Renal Failure Nursing Care PlansMichael Baylon DueñasОценок пока нет
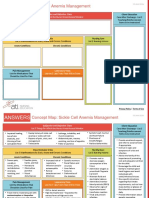
- NCC-SickleCellAnemiaManagement ConceptMap InteractivePDFДокумент2 страницыNCC-SickleCellAnemiaManagement ConceptMap InteractivePDFLoggerz Arck100% (1)
- Intracerebral HemorrageДокумент13 страницIntracerebral HemorrageChristian JuarezОценок пока нет
- Decreased Cardiac Output RM 7Документ9 страницDecreased Cardiac Output RM 7api-283470660Оценок пока нет
- NCM 106 - Case Analysis - Nursing Care Plan of Heart FailureДокумент2 страницыNCM 106 - Case Analysis - Nursing Care Plan of Heart FailureMarisol Jane JomayaОценок пока нет
- Neurogenic ShockДокумент11 страницNeurogenic Shocklulu voxОценок пока нет
- Indication Specific Action Side Effects/ Adverse Effects Nursing Consideration/ Patient TeachingДокумент6 страницIndication Specific Action Side Effects/ Adverse Effects Nursing Consideration/ Patient TeachingKrista Madranca CastroОценок пока нет
- Hemorrhagic Cerebro Vascular DiseaseДокумент37 страницHemorrhagic Cerebro Vascular Diseasejbvaldez100% (1)
- Burns CH 25 n-7Документ7 страницBurns CH 25 n-7Jessica VargasОценок пока нет
- Myocardial InfarctionДокумент18 страницMyocardial InfarctionYanna Habib-MangotaraОценок пока нет
- Cap Grand Case PreДокумент46 страницCap Grand Case PreMatty FelОценок пока нет
- Script For EcgДокумент14 страницScript For EcgMonesa Badil LingasaОценок пока нет
- Complete Guide To ECGДокумент78 страницComplete Guide To ECGAnas YahyaОценок пока нет
- Pharm Exam ReviewДокумент13 страницPharm Exam ReviewAshleyОценок пока нет
- Angina PectorisДокумент8 страницAngina PectorisJoanne LagusadОценок пока нет
- Multiple Injuries: Physical Examination and Review of SystemsДокумент5 страницMultiple Injuries: Physical Examination and Review of SystemsTarquin Tomada100% (1)
- Cardiac TamponadeДокумент3 страницыCardiac Tamponadescremo_xtreme100% (2)
- Nursing Management Pancreatic CancerДокумент2 страницыNursing Management Pancreatic CancerKit NameKo100% (2)
- Types of ShocksДокумент33 страницыTypes of Shocksmark OrpillaОценок пока нет
- Assessment Diagnosis Inference Planning Interventio N Rationale EvaluationДокумент9 страницAssessment Diagnosis Inference Planning Interventio N Rationale Evaluationjosh100% (1)
- Cardiology Case 1Документ2 страницыCardiology Case 1vil62650% (2)
- 19 Cardiac DisordersДокумент51 страница19 Cardiac DisordersChessie Garcia100% (1)
- Coarctation of The AortaДокумент26 страницCoarctation of The AortaMissDyYournurseОценок пока нет
- RevisionДокумент17 страницRevisionMatt RenaudОценок пока нет
- Dysrhythmias NotesДокумент23 страницыDysrhythmias NoteskmimmackОценок пока нет
- Chest TubesДокумент12 страницChest TubesMark Hammerschmidt100% (4)
- Medicine Ward NCPДокумент11 страницMedicine Ward NCPKimsha ConcepcionОценок пока нет
- Multiple MyelomaДокумент5 страницMultiple MyelomaDiane Kate Tobias MagnoОценок пока нет
- ValvularДокумент2 страницыValvularJulia Rae Delos SantosОценок пока нет
- Classification of Burns Based On Depth CharacteristicsДокумент2 страницыClassification of Burns Based On Depth CharacteristicsmexelleОценок пока нет
- Aortic Valve StenosisДокумент4 страницыAortic Valve StenosisYrag NoznipОценок пока нет
- Coronary Artery DiseaseДокумент3 страницыCoronary Artery Diseasetrew_wertОценок пока нет
- Cardiovascular 9. Acute Myocardial InfarctionДокумент39 страницCardiovascular 9. Acute Myocardial Infarctionapi-19641337100% (2)
- Nursing Care PlanДокумент3 страницыNursing Care PlanMarielle SorianoОценок пока нет
- Chest Pain Care PlanДокумент2 страницыChest Pain Care Planapi-545292605Оценок пока нет
- Myocardial InfarctionДокумент28 страницMyocardial Infarctionshaitabligan100% (1)
- Nursing Care PlanДокумент10 страницNursing Care PlanmariasomorayОценок пока нет
- Case Presentation - NSTEMIДокумент18 страницCase Presentation - NSTEMIZОценок пока нет
- Disorder of Respiratory SystemДокумент89 страницDisorder of Respiratory SystemDarine Nasr100% (1)
- Jade R. Dinolan BSN-4: Diagnosi SДокумент5 страницJade R. Dinolan BSN-4: Diagnosi SJhade Relleta100% (1)
- Medical Surgical Nursing Kawasaki DiseaseДокумент2 страницыMedical Surgical Nursing Kawasaki DiseaseChieChay DubОценок пока нет
- CardiomyopathyДокумент2 страницыCardiomyopathyBianca SarmientoОценок пока нет
- Buergers Disease Concept MapДокумент1 страницаBuergers Disease Concept MapElmer Dizon100% (1)
- Lect15&16 Fluids&ElectrolytesДокумент77 страницLect15&16 Fluids&Electrolyteskhurram na100% (1)
- Abdominal Aortic AneurysmДокумент2 страницыAbdominal Aortic AneurysmAria MontgomeryОценок пока нет
- TOF Patient EducationДокумент8 страницTOF Patient EducationMia MiaОценок пока нет
- Cardiovascular Agents: Florianne E. Adlawan, R.NДокумент31 страницаCardiovascular Agents: Florianne E. Adlawan, R.NadlawanflorianneОценок пока нет
- ArteriosclerosisДокумент8 страницArteriosclerosisRhea Liza Comendador-TjernmoenОценок пока нет
- EINC ReviewДокумент14 страницEINC ReviewRifa'atul MahmudahОценок пока нет
- Pathophysiology of ArrhythmiasДокумент15 страницPathophysiology of ArrhythmiasJonathan MontecilloОценок пока нет
- A Simple Guide to Circulatory Shock, Diagnosis, Treatment and Related ConditionsОт EverandA Simple Guide to Circulatory Shock, Diagnosis, Treatment and Related ConditionsОценок пока нет
- A Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsОт EverandA Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsОценок пока нет
- CoA PCICSДокумент13 страницCoA PCICSAdrian KhomanОценок пока нет
- Er Medicine ReviewДокумент16 страницEr Medicine Reviewsdb10cОценок пока нет
- Aortic CoarctationДокумент4 страницыAortic CoarctationFrancois Donatien De SadeОценок пока нет
- Crops Fruits of Warm Climates 2004Документ2 997 страницCrops Fruits of Warm Climates 2004Helmy Momogi SyadianОценок пока нет
- Crops Fruits of Warm Climates 2004Документ2 997 страницCrops Fruits of Warm Climates 2004Helmy Momogi SyadianОценок пока нет
- Typhimurium) : Kusdalinah, Andrew Johan, Noor WijayahadiДокумент5 страницTyphimurium) : Kusdalinah, Andrew Johan, Noor WijayahadiHelmy Momogi SyadianОценок пока нет
- AHA/CDC Scientific Statement: Markers of Inflammation and Cardiovascular DiseaseДокумент13 страницAHA/CDC Scientific Statement: Markers of Inflammation and Cardiovascular DiseaseHelmy Momogi SyadianОценок пока нет
- MCQS CardiologyДокумент40 страницMCQS CardiologyWaleed SofiОценок пока нет
- (Contemporary Neurology Series) Robert B. Darnell, Jerome B. Posner-Paraneoplastic Syndromes-Oxford University Press (2011)Документ497 страниц(Contemporary Neurology Series) Robert B. Darnell, Jerome B. Posner-Paraneoplastic Syndromes-Oxford University Press (2011)Pedro BarrosОценок пока нет
- Wilson, R. L., & Stevenson, C. E. (2019) - Anatomy and Physiology of The Stomach. Shackelford's Surgery of The Alimentary Tract, 2 Volume SetДокумент14 страницWilson, R. L., & Stevenson, C. E. (2019) - Anatomy and Physiology of The Stomach. Shackelford's Surgery of The Alimentary Tract, 2 Volume SetanastasijaОценок пока нет
- Antenatal Assessment of Fetal Well-BeingДокумент18 страницAntenatal Assessment of Fetal Well-BeingAmritaОценок пока нет
- Introduction To Critical Care NursingДокумент10 страницIntroduction To Critical Care NursingAngielyn Ramos Oloraza100% (2)
- Cystic Diseases of KidneyДокумент12 страницCystic Diseases of Kidneymnr hmcОценок пока нет
- Bahasa Inggris - 12 SMA PTN Worksheet 2 (Report, Caption,.Документ7 страницBahasa Inggris - 12 SMA PTN Worksheet 2 (Report, Caption,.Jiansyah AbdullahОценок пока нет
- Chapter 2 - Examination of Vital SignsДокумент85 страницChapter 2 - Examination of Vital SignsAudrrey LewisОценок пока нет
- Cardiovascular Safety of Anti-Diabetic Drugs - KarklinДокумент42 страницыCardiovascular Safety of Anti-Diabetic Drugs - KarklinCharles SaputraОценок пока нет
- Gout and HyperuricemiaДокумент70 страницGout and HyperuricemiaThe AbyssinicansОценок пока нет
- Ebook Harrisons Pulmonary and Critical Care Medicine 3E PDF Full Chapter PDFДокумент67 страницEbook Harrisons Pulmonary and Critical Care Medicine 3E PDF Full Chapter PDFnancy.stice552100% (24)
- Heart Failure in Dogs: 6 Practical Tips From CardiologistsДокумент6 страницHeart Failure in Dogs: 6 Practical Tips From CardiologistsJessareth Atilano CapacioОценок пока нет
- Osmosis High-Yield Physiology - Medicalstudyzone - Com (Sürüklenen)Документ87 страницOsmosis High-Yield Physiology - Medicalstudyzone - Com (Sürüklenen)Dilay MercimekОценок пока нет
- 5P MEDICINE2 Valvular Heart Disease 1 - Dr. Rene ManaloДокумент6 страниц5P MEDICINE2 Valvular Heart Disease 1 - Dr. Rene Manalok.n.e.d.Оценок пока нет
- Subclinical Thyroid Dysfunction: Diagnosis and Management: Budiman Darmowidjojo, Lucia Dwi AntikaДокумент11 страницSubclinical Thyroid Dysfunction: Diagnosis and Management: Budiman Darmowidjojo, Lucia Dwi AntikaMuhammad Reyhan HidayatОценок пока нет
- Effect of Increasing Age On Cataract Surgery OutcoДокумент4 страницыEffect of Increasing Age On Cataract Surgery OutcoKanneaufii KaramelОценок пока нет
- Non-Invasive Ventilation 2Документ25 страницNon-Invasive Ventilation 2Ramanesh DОценок пока нет
- EnalaprilДокумент2 страницыEnalaprilpinksapphire929100% (2)
- UntitledДокумент1 089 страницUntitledMasoud AbsalanОценок пока нет
- Cardiac Enzyme StudiesДокумент4 страницыCardiac Enzyme StudiesDara VinsonОценок пока нет
- NCMB ReviewerДокумент9 страницNCMB Reviewer5S CASTILLEJO Danica M.Оценок пока нет
- Drug Presentation On Morphine SulphateДокумент38 страницDrug Presentation On Morphine SulphateBHUVAN KUMAR. TОценок пока нет
- Stroke RehabilitationДокумент57 страницStroke RehabilitationWahyu FajarОценок пока нет
- Lesson Plan On DeliriumДокумент5 страницLesson Plan On DeliriumAnkush Kulat PatilОценок пока нет
- Antenatal Care Unit Two Lesson 192Документ192 страницыAntenatal Care Unit Two Lesson 192RidiculouslySweetОценок пока нет
- FicatulДокумент107 страницFicatulkoxОценок пока нет
- Atrioventricular Nodal Reentry Tachycardia (AVNRT)Документ24 страницыAtrioventricular Nodal Reentry Tachycardia (AVNRT)Radya Agna100% (1)
- DrowningДокумент28 страницDrowningjparker35045Оценок пока нет
- Salisbury 1100 Harrison PDFДокумент62 страницыSalisbury 1100 Harrison PDFDrNaveen Singh Rajpurohit KaduОценок пока нет
- Study Guide For The ATLS ManualДокумент41 страницаStudy Guide For The ATLS ManualCarl Sars100% (2)